
Initial Workup
- Labs: CBC, BMP, LFTs, TSH, HIV, ANA, BNP, troponin
- V/Q scan: rule out CTEPH (Group 4)
- PFTs, Oximetry, HRCT: if ILD or OSA suspected
- Diuresis
- Oxygen goal: >92%
PH Classification
| Group | Etiology | Examples | Workup | Treatment |
|---|---|---|---|---|
| 1 | PAH | Idiopathic, CTD, HIV, drugs | ANA, HIV, LFTs, RHC (pre-capillary), V/Q scan | ERA, PDE5i, prostacyclins, diuretics, O2, CCB if vasoreactive |
| 2 | Left Heart Disease | HFrEF, HFpEF, valvular disease | TTE, BNP, RHC (post-capillary, wedge > 15) | Optimize HF, ACEi/ARB, BB, diuretics, valve repair/replacement |
| 3 | Lung Disease / Hypoxia | COPD, ILD, OSA, altitude | PFTs, oximetry, ABG, HRCT | Oxygen if hypoxic, treat lung disease, PAH meds usually not indicated |
| 4 | CTEPH | Prior PE, thrombophilia | V/Q scan, CT PA, RHC | Anticoagulation, PTE surgery, riociguat, BPA if inoperable |
| 5 | Multifactorial | Sarcoid, sickle cell, CKD | Tailored labs, imaging, biopsies | Treat underlying disease, PAH therapies case-by-case |
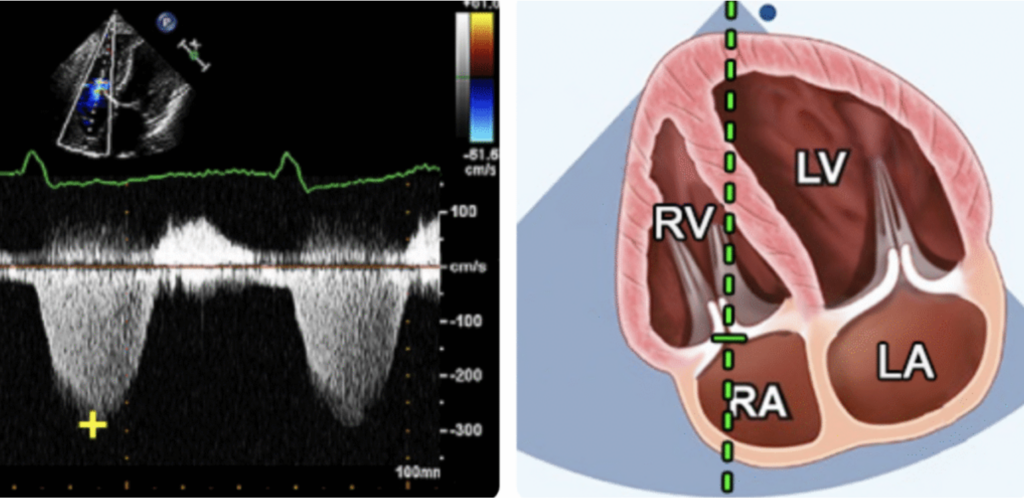
Gold standard to define PH is a mPAP > 20mmHg on right heart cath, but TTE has its utility - it is around 85% sensitive and 70% specific for detecting the presence of PH. TTE parameters that are measured are the following:
- Elevated systolic PA pressure (sPAP)
- Right heart dilation or dysfunction
- TR jet velocity >2.8 m/s
- Signs of right heart strain
PH Severity by RHC & TTE
| Severity | mPAP (RHC) | sPAP (TTE) |
|---|---|---|
| Normal | ≤ 20 mmHg | < 35 mmHg |
| Mild PH | 21–30 mmHg | 35–44 mmHg |
| Moderate PH | 31–40 mmHg | 45–59 mmHg |
| Severe PH | > 40 mmHg | ≥ 60 mmHg |
TTE Measurements
- Estimated RAP: 3-15mmHg based on IVC diameter and collapsibility: If <2.1cm and >50% collapse = 3mmHg, If >2.1cm or <50% collapse = 8mmHg, if >2.1cm and <50% collapse = 15mmHg
- TR peak velocity: ≥2.8 m/s → Suggests elevated pulmonary pressures
- Estimated RVSP: RVSP ≈ 4 × (TR peak velocity)² + RAP
- PH severity: Mild (35–44 mmHg), moderate (45–59 mmHg), or severe (≥60 mmHg)
RVSP Calculator
RVSP Severity Reference
| RVSP | Interpretation |
|---|---|
| < 35 mmHg | Normal |
| 35–44 mmHg | Mild PH |
| 45–59 mmHg | Moderate PH |
| ≥ 60 mmHg | Severe PH |
RHC Measurements
- PCWP (wedge pressure)
- ≤15 mmHg = pre-capillary (Groups 1, 3, 4)
- 15 mmHg = post-capillary (Group 2)
- PVR
- ≥3 Wood units + high PAWP = combined pre- and post-capillary (Group 2/5 overlap)
Pulmonary HTN Severity + PVR Calculator
mPAP Severity Reference
| mPAP (RHC) | Interpretation |
|---|---|
| ≤ 20 mmHg | Normal |
| 21-30 mmHg | Mild elevation |
| 31-40 mmHg | Moderate elevation |
| > 40 mmHg | Severe elevation |
PVR Severity Reference
| PVR | Interpretation |
|---|---|
| < 2 WU | Normal |
| 2.0-2.9 WU | Mild elevation |
| 3.0-5.0 WU | Moderate elevation |
| > 5.0 WU | Severe elevation |
PVR = (mPAP - PCWP) / CO
Group 1 (Pulmonary Arterial Hypertension – PAH)
Etiologies: idiopathic, connective tissue disease, HIV, drugs
Treatment:
- PDE-5 inhibitors: sildenafil 20 mg TID, tadalafil 40 mg daily
- Endothelin receptor antagonists: ambrisentan, macitentan
- sGC stimulator: riociguat 1–2.5 mg TID (avoid with PDE5i)
- Prostacyclins: epoprostenol (IV), treprostinil
- Consider vasoreactivity testing → CCBs if positive
- Refer to PH specialty center for advanced therapies