
Acute Pancreatitis
Confirm diagnosis
2 of 3: pain, lipase ≥3x ULN, imaging
Initial management (first 24h)
LR bolus → then ~1.5 cc/kg/hr
Opioids for pain
NPO initially
Opioids for pain
NPO initially
Severity
Organ failure, shock, hypoxemia?
Yes → ICU
No → Floor + close reassessment
Yes → ICU
No → Floor + close reassessment
Etiology-driven actions
Gallstones → RUQ US → ERCP if cholangitis/obstruction
Triglycerides >1000 → insulin infusion ± plasmapheresis
Alcohol → supportive + withdrawal mgmt
Meds → stop offending agent
Triglycerides >1000 → insulin infusion ± plasmapheresis
Alcohol → supportive + withdrawal mgmt
Meds → stop offending agent
Fluids reassessment (q6–12h)
Check BUN, Cr, Hct, UOP
Rising BUN or low UOP → give more fluid
Hypoxia/effusions → slow fluids
Rising BUN or low UOP → give more fluid
Hypoxia/effusions → slow fluids
Can tolerate PO?
Pain improving, no vomiting
Yes
Start low-fat diet early
Good response
Advance diet → discharge when stable
No
Unable to tolerate by 48–72h
Next step
Enteral feeds (NG/NJ)
Avoid TPN
Avoid TPN
Complications or worsening?
Persistent SIRS >48h → CT
Infected necrosis → antibiotics + drainage
Pseudocyst → treat if symptomatic
Infected necrosis → antibiotics + drainage
Pseudocyst → treat if symptomatic
Consults
GI → ERCP
IR → drainage
Surgery → complications or unclear dx
IR → drainage
Surgery → complications or unclear dx
Diagnosis
Acute pancreatitis is diagnosed when 2 of 3 are present
- Typical epigastric pain, often radiating to the back
- Lipase or amylase at least 3 times ULN
- Imaging findings consistent with pancreatitis
Causes
- Most cases are from gallstones or alcohol
- But also consider triglycerides, medications, hypercalcemia, post-ERCP, trauma, infection, autoimmune disease, and malignancy
Initial workup
- CBC, CMP, LFTs, lipase
- Triglycerides
- Calcium
- RUQ ultrasound if biliary cause possible
- CT only if diagnosis unclear, severe disease suspected, or not improving
- Review meds and recent ERCP history
Severity
- BISAP score
- SIRS, hypotension, rising BUN/Cr
- Hypoxemia or pleural effusions
- Hemoconcentration
- Organ failure or persistent severe pain/vomiting
BISAP Score
Bedside Index for Severity in Acute Pancreatitis. One point for each item present in the first 24 hours.
0
Lower risk
Usually lower short-term mortality risk. Still reassess frequently for evolving organ failure, rising BUN/Cr, hypoxemia, or worsening pain.
Management
- LR preferred for early fluid resuscitation
- Give enough fluid early, then reassess often and avoid overload
- Opioids okay if needed for pain control
- Start oral feeding early once tolerated, usually low fat
- No routine antibiotics unless infected necrosis or another infection is suspected
- ERCP urgently if cholangitis or persistent biliary obstruction
- ICU if shock, respiratory failure, severe AKI, or persistent organ failure
Hypertriglyceridemia pancreatitis
- Suspect if TG >1000 (risk ↑ >2000), milky serum, or pancreatitis with normal amylase
- Common in diabetes, alcohol use, obesity, pregnancy, estrogen meds
- Mechanism: TG → free fatty acids → pancreatic injury + ischemia
Management
- LR fluids
- Insulin infusion (0.1 u/kg/hr ± dextrose) → goal TG <500
- Monitor glucose, K closely
- Consider plasmapheresis if severe or TG extremely high
Prevention
- Fibrate first-line
- ± omega-3
- Glycemic control
- Low-fat diet + alcohol cessation
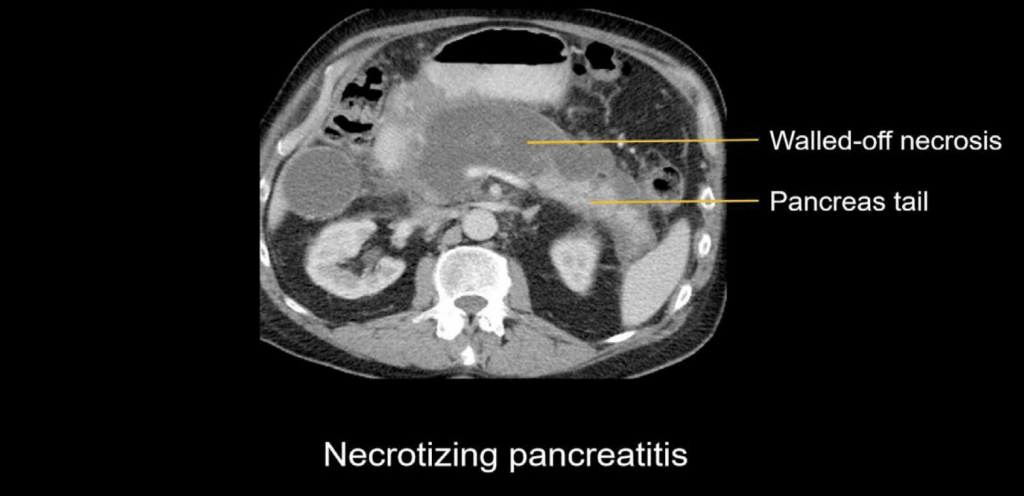
Complications
- Necrosis
- Pseudocyst or walled-off necrosis
- ARDS
- AKI
- Hypocalcemia
- Abdominal compartment syndrome
- Splenic or portal vein thrombosis
Trials
Aggressive vs Moderate Fluids (WATERFALL) - 2022
- RCT (n=249) acute pancreatitis
- Aggressive: 20 cc/kg bolus + 3 cc/kg/hr vs Moderate: selective bolus + 1.5 cc/kg/hr
- No reduction in moderately severe/severe pancreatitis
- ↑ fluid overload (20.5% vs 6.3%) → trial stopped early
- Takeaway: avoid aggressive upfront fluids, use moderate/goal-directed approach
Goal-directed fluids: LR vs NS - 2011
- Small RCT (~40 pts) comparing LR vs NS
- LR ↓ SIRS (84% vs 0%) and ↓ CRP
- Likely due to less hyperchloremic acidosis vs NS
- Takeaway: LR preferred initial fluid in pancreatitis