
Background & workup
- Microcytosis and hypochromasia, with MCV <80 fL
- Symptoms include fatigue, weakness, pagophagia (craving ice), and dyspnea on exertion
- Assess for sources of bleeding (GI, menstrual, etc.), malabsorption (celiac disease), or a family history of anemia
- Menstrual history is crucial in reproductive-age women, as heavy bleeding is a common cause
- GI workup: Consider in men, postmenopausal women, or cases with GI symptoms or family history of colon cancer
Suspected iron deficiency
Obtain ferritin with or without iron studies
(iron, TIBC, calculated TSAT)
Is the ferritin low?
(iron, TIBC, calculated TSAT)
Is the ferritin low?
Yes
No
Iron deficiency confirmed
- Treat with iron
- Identify source of deficiency or blood loss
- Confirm response after treatment
Is the TSAT low?
Yes
No
Iron deficiency confirmed
- Treat with iron
- Identify source of deficiency or blood loss
- Confirm response after treatment
Iron deficiency unlikely but possible
- Consider specialized testing if suspicion remains high
- Evaluate other causes of anemia or symptoms
Key labs
- Hemoglobin & MCV: Helps differentiate between IDA, thalassemia, anemia of chronic disease, and sideroblastic anemia
- Mentzer Index: MCV/RBC count. <13 suggests thalassemia, >16 suggests IDA
- Reticulocyte Count: Low (<2%) in IDA, higher in bleeding or hemolysis
- Ferritin: Best indicator of iron stores. IDA is likely if <30 mcg/L, though inflammatory states can elevate ferritin
- TIBC, Iron Saturation, RDW: Less specific but can support diagnosis
Mentzer Index
When to treat
- Treat if Hgb < 13 g/dL in men and < 12 g/dL in nonpregnant women
- Treat if ferritin < 45 ng/mL or TSAT <= 20%
Management
Adult with iron deficiency
Severe or life-threatening anemia?
Yes
Transfuse RBCs
Give iron after stabilization
No
IV iron indications?
- Oral failure or intolerance
- Surgery soon
- IBD
- Bariatric or gastrectomy
- Dialysis
Yes
IV iron preferred
No
Oral iron preferred
QD or alternate days
Diet & oral iron
- Diet: Iron from meat is better absorbed than plant sources. Avoid spinach, coffee, and tea near iron intake
- Oral Iron: Ferrous sulfate preferred (325mg EOD); alternatives include ferrous gluconate or ferrous bisglycinate
- Dosing: Once daily preferred. Alternate-day dosing may reduce GI side effects but is harder to remember
- Vitamin C: May enhance iron absorption but not always necessary
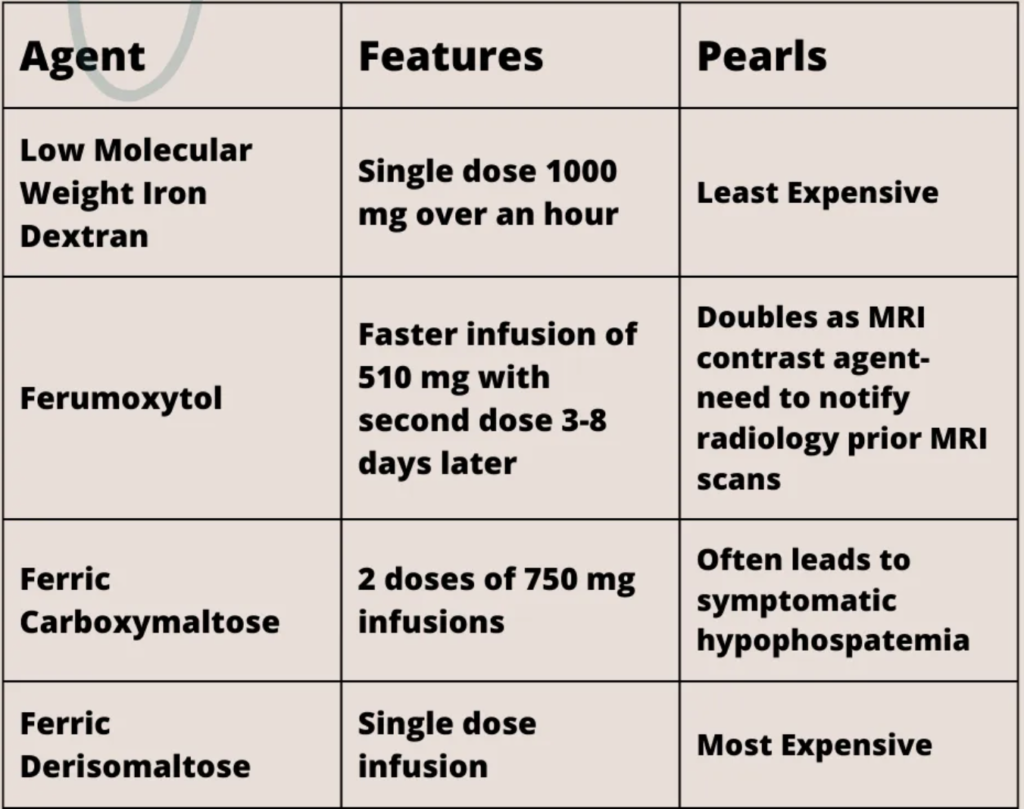
IV iron
- Indicated for intolerance to oral iron, malabsorption (IBD, bariatric surgery), or severe deficiency
- Iron dextran: Single 1000 mg dose
- Ferumoxytol: Rapid infusion, affects MRI readings
- Ferric carboxymaltose: Risk of severe hypophosphatemia
- Ferric derisomaltose: Single-dose option
- Reactions: Usually non-IgE-mediated; premedication needed for high-risk patients
Monitoring/special considerations
- Oral Iron: Check Hgb and ferritin at 3 months
- IV Iron: Check ferritin at 1 month, then every 3 months. Repeat IV iron if ferritin <50
- Restless Leg Syndrome (RLS): Aim for ferritin >75 mcg/L
- Alopecia: Iron supplementation may help in iron-related hair loss
- Anemia of Chronic Disease: Often requires IV iron due to hepcidin-mediated iron sequestration
- Refer to heme if recurrent need for IV iron, diagnostic uncertainty