
Overview
Idioventricular rhythms originate from ventricular tissue when higher pacemakers (SA or AV nodes) fail or when ventricular automaticity increases. They present as wide-complex rhythms, often with absent or dissociated P waves. These rhythms can be protective (escape) or pathologic (VT).
Types
- Idioventricular Rhythm: 20–40 bpm (ventricular escape)
- Accelerated Idioventricular Rhythm (AIVR): 40–100 bpm, often post-reperfusion after MI
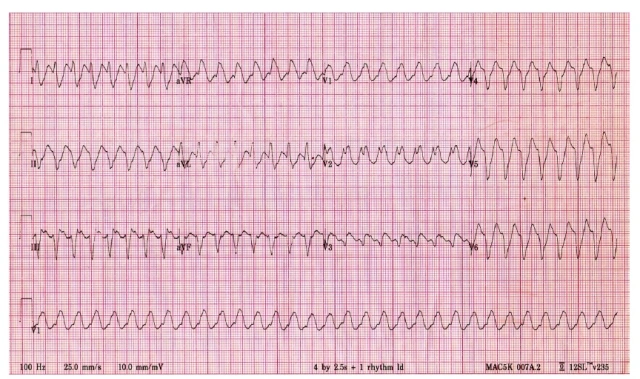
- Ventricular Tachycardia (VT): >100 bpm, pathologic, may be unstable
Causes
- MI (especially reperfusion phase)
- Severe sinus node dysfunction or high-grade AV block
- Drug toxicity (digoxin, antiarrhythmics)
- Myocarditis or cardiomyopathy
EKG
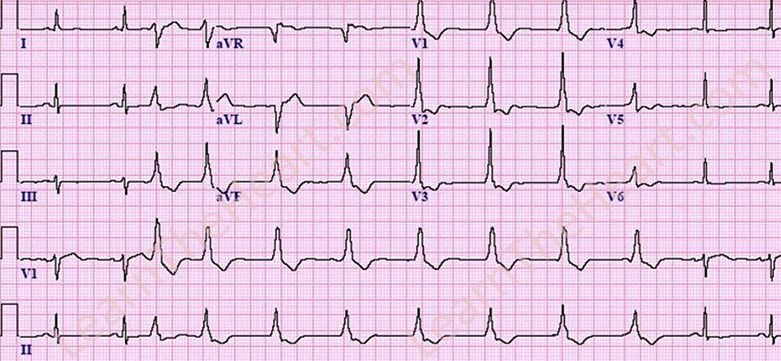
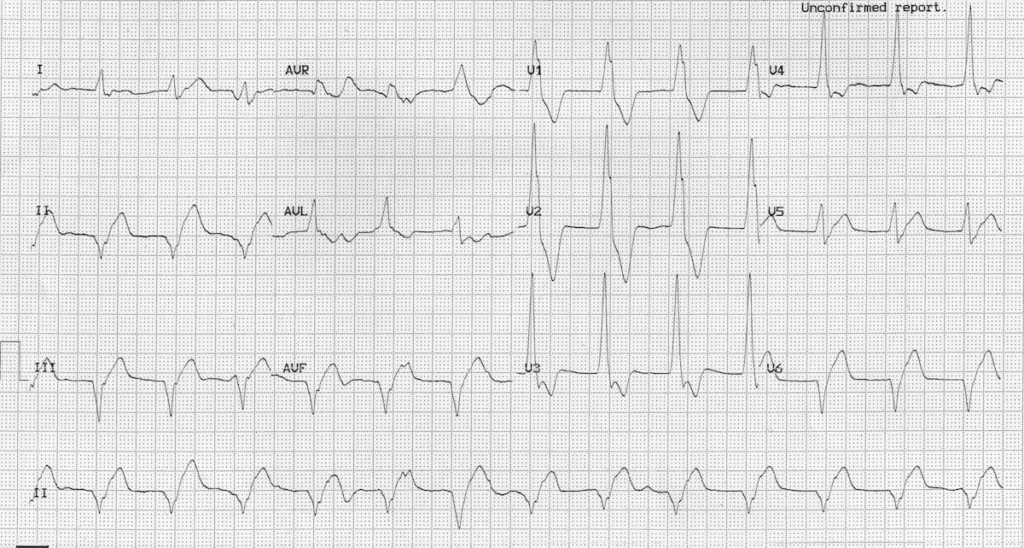
- Wide QRS (>120 ms)
- Rate corresponds to type (20–40, 40–100, or >100 bpm)
- AV dissociation or absent P waves
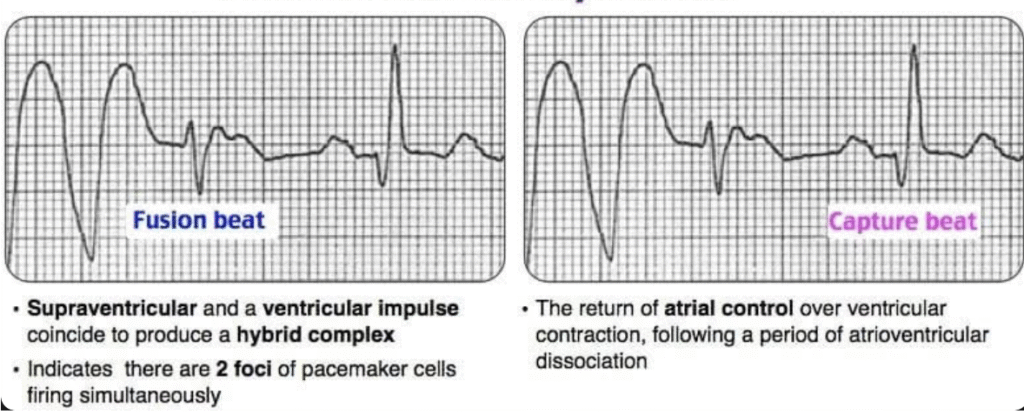
- Possible capture (normal SA node beat) or fusion beats (SA node and ventricle contract at same time)
Clinical Significance
- Idioventricular escape rhythms are generally protective and do not require treatment if asymptomatic
- AIVR is usually transient and self-limited, commonly seen post-reperfusion
- Sustained VT is pathologic and may cause hemodynamic compromise, requiring immediate intervention
Management
- Address underlying cause (ischemia, electrolytes, drug toxicity)
- Idioventricular escape rhythms: no therapy if stable
- AIVR: usually observation only
- VT: manage per ACLS (unstable → cardioversion; stable → antiarrhythmics)