
Overview
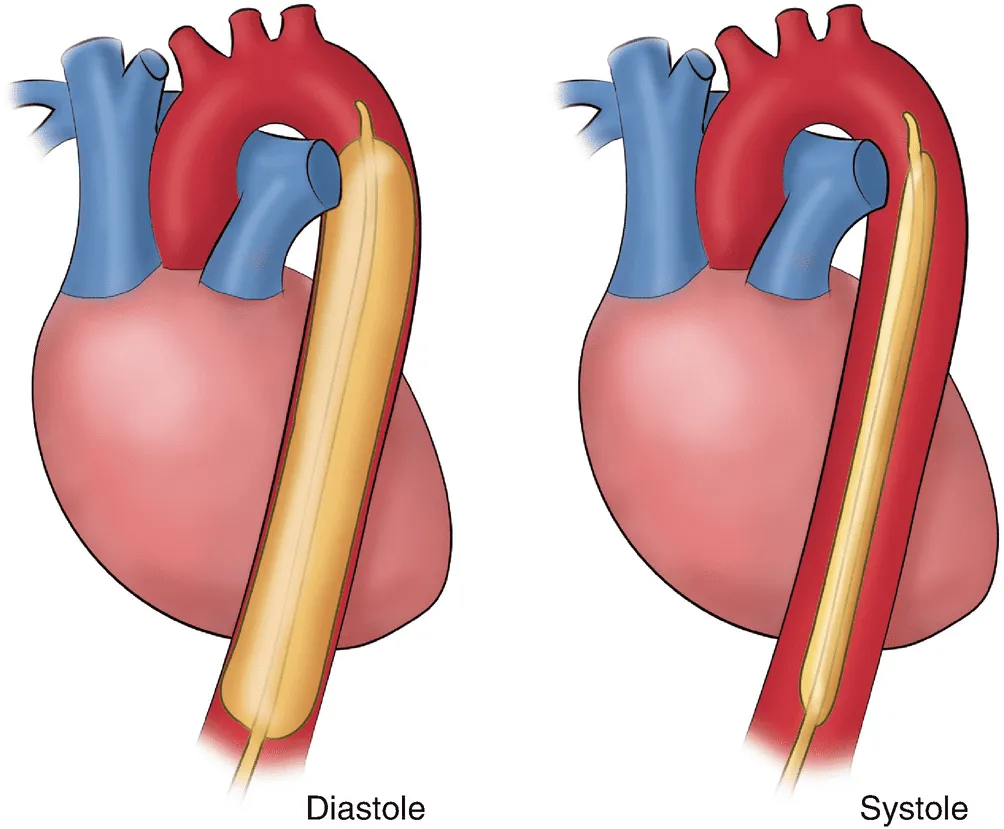
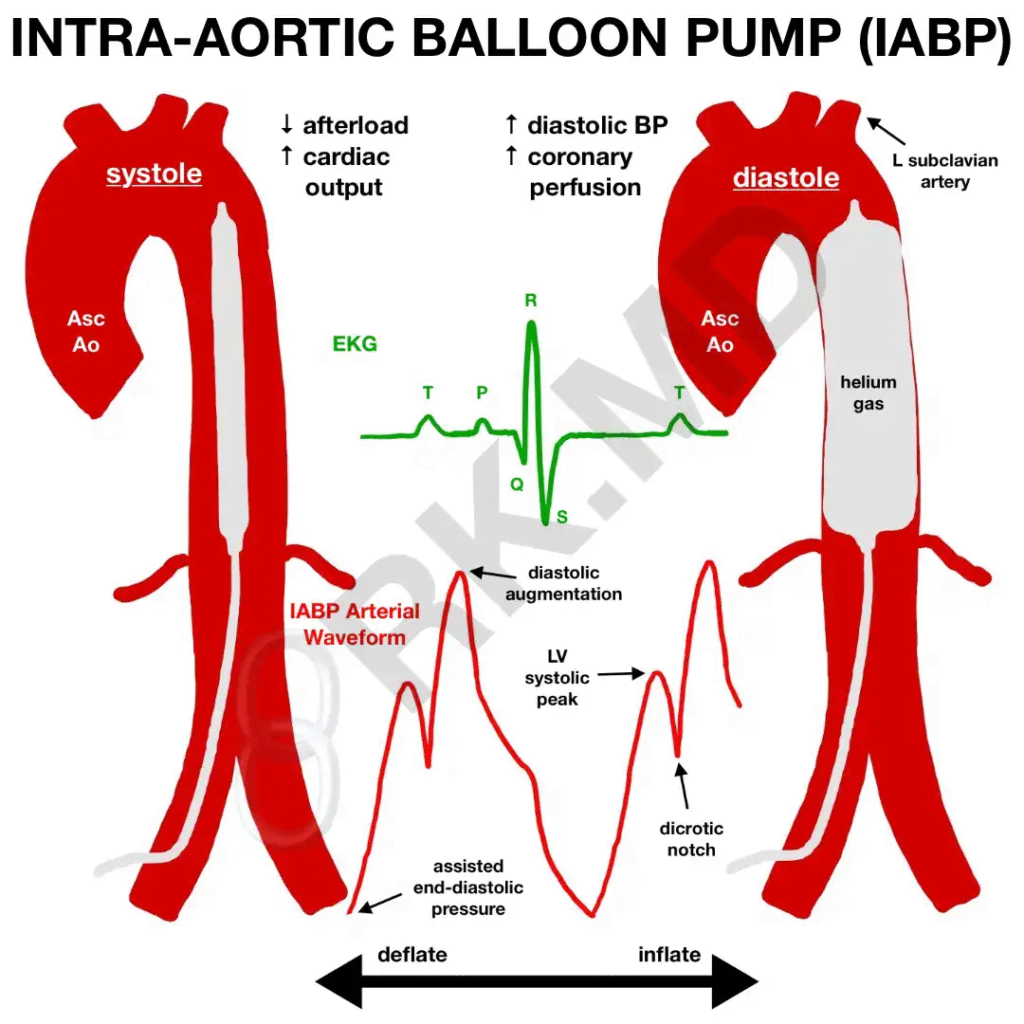
IABP is a percutaneous counterpulsation device that inflates during diastole to raise coronary perfusion and deflates just before systole to lower afterload and improve forward flow.
- Trigger: ECG or arterial line
- Helium-filled balloon
- Typically inserted via femoral access
Indications
- Cardiogenic shock (especially acute MI) as a bridge to PCI, CABG, or definitive therapy
- Post-cardiotomy low output state
- Refractory ischemia/unstable angina awaiting revascularization
- Mechanical complications of MI (MR from papillary rupture, VSD) — temporary stabilization
- High-risk PCI requiring hemodynamic support
- Acute decompensated HFrEF with low output despite therapy
Pearls:
- Most benefit when ischemia is active and SVR is high
- Always a bridge to something: revascularization, recovery, or durable MCS — never destination therapy
Contraindications
Absolute
- Moderate to severe aortic regurgitation
- Aortic dissection
- Severe PAD preventing femoral access
Relative
- Uncontrolled bleeding or coagulopathy
- Aortic aneurysm with mural thrombus
- Severe sepsis or profound vasodilation
- Severe uncontrolled hypertension
How It Helps
- Diastolic augmentation: Balloon inflates during diastole, raising aortic diastolic pressure → improved coronary perfusion
- Afterload reduction: Rapid deflation just before systole → reduced LV wall stress and myocardial O₂ demand, improved stroke volume
- Net effect: ↑ MAP, ↑ oxygen delivery, modest ↑ cardiac output, ↓ LVEDP
Placement & Position
Sizing & Insertion
- Balloon sizes: 34–50 cc (based on patient height)
- Usually inserted via femoral access under fluoroscopy
- Anticoagulation commonly used unless contraindicated
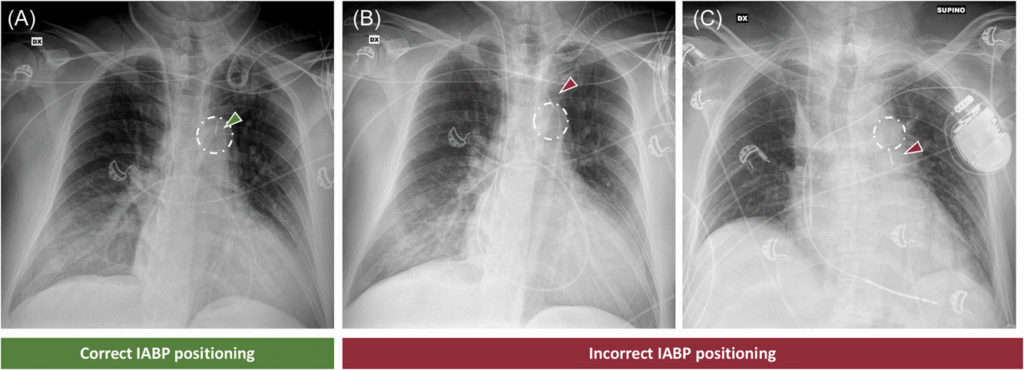
Correct Position
- Tip 2–3 cm distal to the left subclavian artery
- Distal balloon above the renal arteries
- On CXR, radiopaque marker near the aortic knob or carina
Post-Placement Checklist:
- Confirm position on fluoro or CXR
- Frequent limb and neurovascular checks (DP/PT pulses, color, temperature)
- Document augmentation %, assist ratio, trigger, and timing
- Set anticoagulation plan and monitor platelets daily
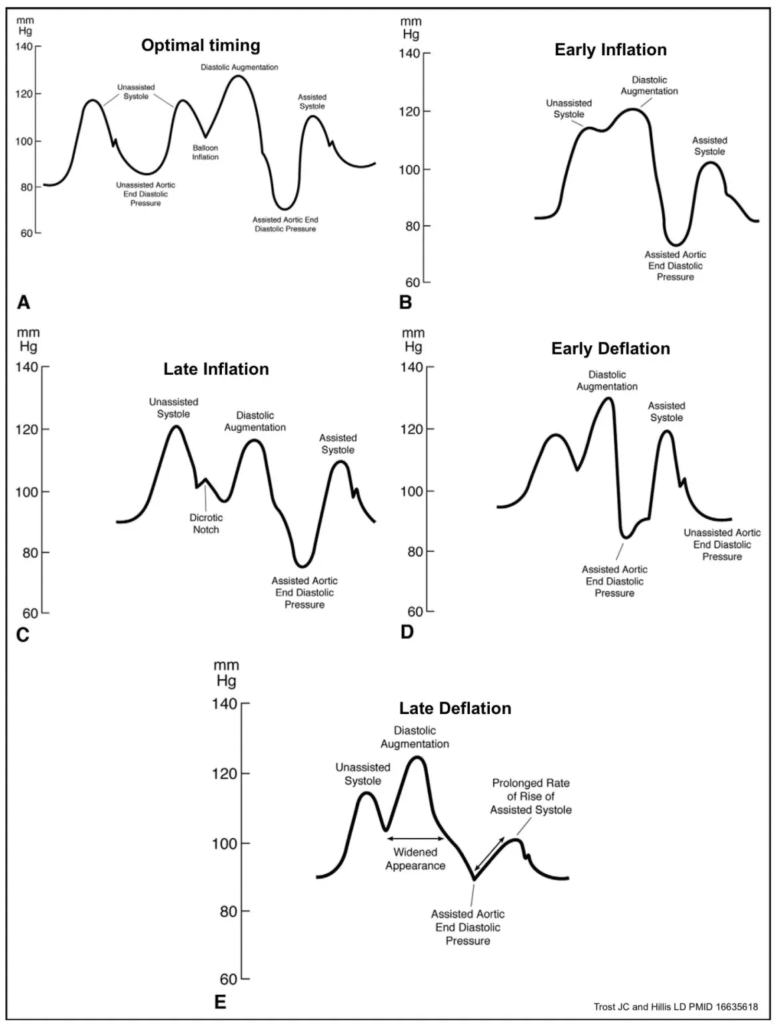
Timing & Augmentation
Goals
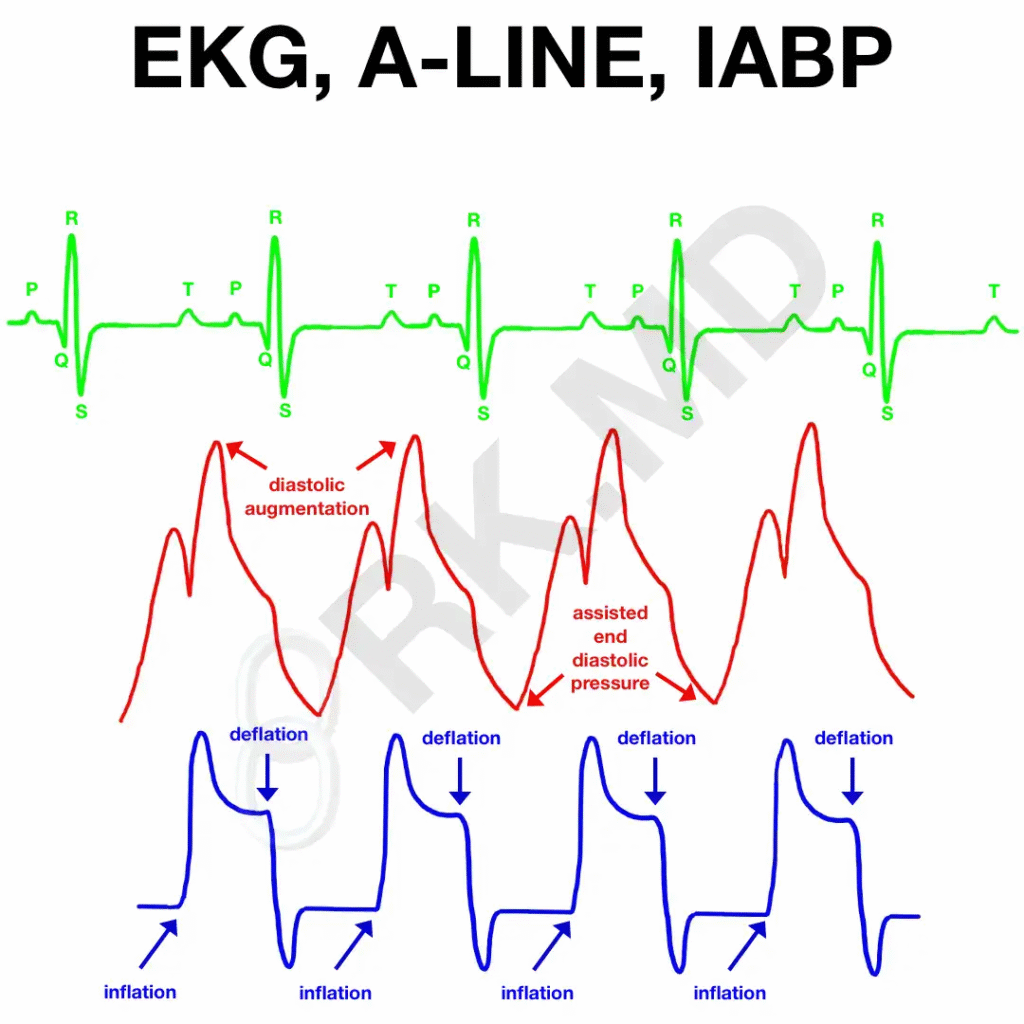
- Inflate: at the dicrotic notch (start of diastole)
- Deflate: just before systole (prior to the upstroke or R-wave)
- Augmented diastolic pressure should exceed unassisted systolic pressure
Controller Basics
- Assist ratio: start 1:1; decrease to 1:2 or 1:3 for weaning
- Augmentation: titrate based on MAP, CI, lactate, and urine output
- Triggering: ECG preferred if stable; switch to arterial trigger if arrhythmias present
| Problem | What You See | Fix |
|---|---|---|
| Late inflation | Small ADP, notch after diastole | Inflate earlier |
| Early inflation | Encroaches on systole | Delay inflation |
| Late deflation | High EDP, widened upstroke | Deflate earlier |
| Early deflation | Loss of diastolic augmentation | Delay deflation slightly |
Waveform: What to Look For
- Augmented diastolic peak higher than native systolic peak
- Assisted end-diastolic pressure lower than unassisted end-diastolic pressure
- Proper timing aligned with cardiac cycle
- Sharp assisted systolic upstroke with correct deflation
Troubleshooting
Common Alarms & Fixes
- Gas leak: ↓ augmentation, repeated auto-fill → stop pump, check tubing, consider exchange
- Balloon rupture: blood in tubing or hematuria → stop pump, clamp catheter, remove balloon
- Poor triggering: switch between ECG and pressure triggers, adjust filters/gain, manage arrhythmias
- Loss of augmentation: verify position, adjust timing, assess MAP/SVR, confirm balloon size and gas volume
Malposition Clues:
- Arm ischemia → balloon too proximal (occluding left subclavian)
- Abdominal pain or decreased urine output → balloon too distal (renal/visceral compromise)
- New neuro changes → possible embolism or migration; image urgently
Complications & Monitoring
- Limb ischemia
- Access-site bleeding or hematoma
- Stroke or systemic embolism
- Thrombocytopenia, hemolysis
- Infection
- Balloon rupture
Monitoring Bundle:
- Neurovascular checks every 1–2 hours
- Daily platelets; monitor Hgb, LDH, haptoglobin if hemolysis suspected
- Hourly urine output; monitor for hematuria
- Inspect access site for bleeding or hematoma
- Follow anticoagulation protocol
Weaning
- Criteria: stable MAP without high-dose pressors, improving lactate, no active ischemia
- Reduce assist ratio gradually: 1:1 → 1:2 → 1:3, monitoring CI, MAP, and perfusion
- Remove once stable at 1:3 on minimal support
- Post-removal: apply manual pressure or closure device, continue frequent limb checks