
TTE Morphology
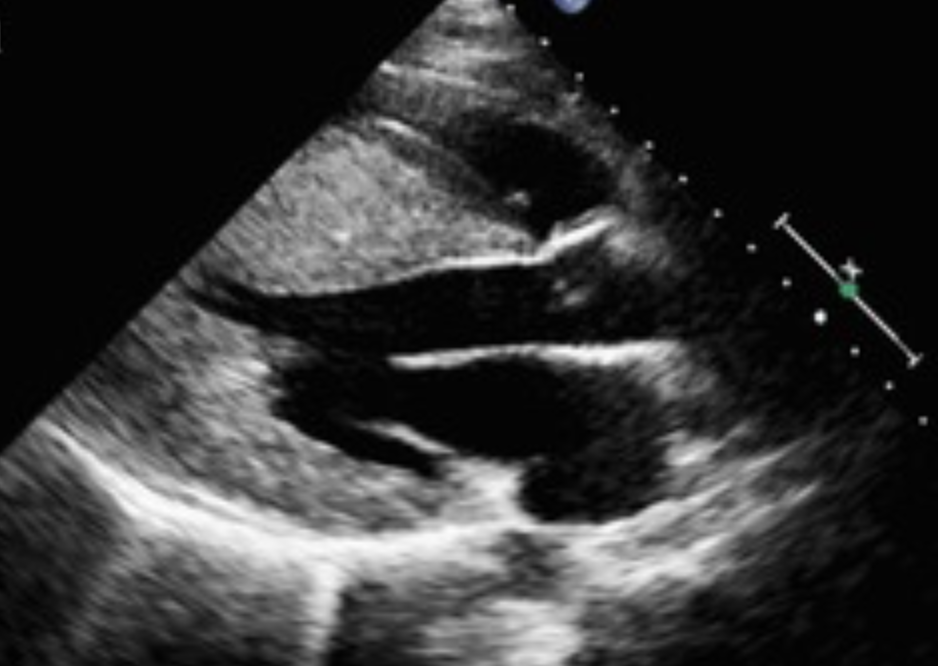
Look for asymmetric septal hypertrophy, small hyperdynamic LV cavity, elongated MV, abnormal papillary muscles, and LAE
Look for Dynamic Obstruction
Assess for SAM - then interrogate the LVOT with Doppler
Interpret the Doppler Pattern
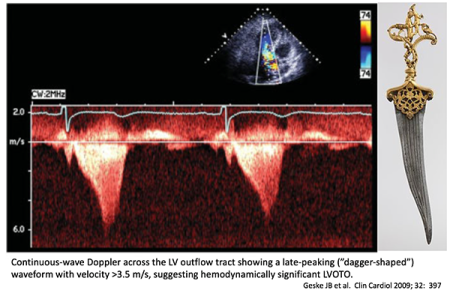
Late-peaking dagger-shaped CW Doppler supports dynamic LVOT obstruction rather than AS
Measure Resting and Provoked Gradient
If resting gradient is low, use Valsalva
Obstructive HCM Pattern
SAM plus significant resting or provoked LVOT gradient, often with posteriorly directed MR
Nonobstructive HCM Pattern
Hypertrophic phenotype present, but no major resting or provoked LVOT gradient
Mitral Valve / MR
Look for SAM-related MR and leaflet or papillary muscle abnormalities
Diastolic Burden
Assess LA size and diastolic dysfunction
Exclude Mimics
Differentiate from AS, hypertensive LVH, sigmoid septum, and subaortic membrane
What you are measuring
- In A5C, A3C and subcostal views
- Peak instantaneous LVOT gradient using CW Doppler
- Convert velocity to gradient: Peak ΔP (mmHg) = 4 × (Vmax in m/s)²
- Report rest and provoked values, and specify the provocation method
How to acquire it correctly
- Use color Doppler first to locate aliasing/turbulence in LVOT
- Place CW Doppler cursor through LVOT, aligned as parallel to flow as possible
- Sweep multiple windows and pick the highest Vmax (best aligned, cleanest envelope)
- Optimize settings: higher sweep speed, appropriate gain to avoid blooming, avoid under-gaining (you will clip the peak)
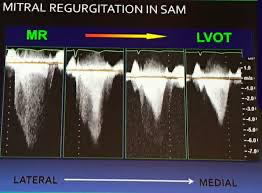
How to confirm it is LVOT and not MR
- LVOT obstruction: “dagger-shaped” late-peaking systolic CW envelope
- MR: denser, often earlier-peaking signal that extends into/through systole (may appear more holosystolic), usually higher velocity than LVOT
- If unsure, compare timing and shape, and correlate with color jet direction and MR severity
- Use PW Doppler mapping: step from LVOT toward apex to localize the site of acceleration (helps distinguish mid-cavity vs LVOT)
What to report
- Resting LVOT Vmax and peak gradient (mmHg)
- Provoked LVOT Vmax and peak gradient, plus provocation method
- Presence/absence of SAM of MV and severity of MR (qualitative is fine)
- If mid-cavity obstruction: state location and report peak gradient there (and clarify it is mid-cavity, not LVOT)
| Category | Peak Gradient (mmHg) |
|---|---|
| Normal | <10 |
| Borderline | 10–30 |
| Abnormal (non-obstructive) | 30–49 |
| Obstructive (clinically significant) | ≥50 (rest or provoked) |
Provocative Testing
- Valsalva or exercise can unmask gradients ≥50 mmHg in symptomatic patients
- These thresholds guide decisions for septal reduction therapies
SAM
Left ventricular outflow tract obstruction occurs when fast-flowing blood through the LV outflow tract pulls the mitral valve anteriorly due to a Venturi effect. This phenomenon is called systolic anterior motion (SAM) of the mitral valve.
SAM leads to 2 key consequences
- Outflow obstruction
- The anteriorly displaced mitral valve obstructs the LV outflow tract
- This impairs systolic ejection into the aorta, reducing cardiac output
- Can lead to hypotension or cardiogenic shock
- Mitral regurgitation
TTE
- Septal hypertrophy (often asymmetric, IVS ≥15 mm)
- Systolic anterior motion (SAM) of mitral valve
- Dynamic obstruction: Late-peaking “dagger-shaped” continuous-wave Doppler curve
- Mitral regurgitation: Posteriorly directed jet due to SAM
- Hyperkinetic LV: Often with near obliteration of the left ventricular cavity during systole
- FH SCD
- Massive LVH
- Unexplained syncope
- Apical aneurysm
- EF ≤50%