
Fascicular Block Algorithm
LAFB pattern
- LAD
- qR in I / aVL
- rS in II / III / aVF
- QRS normal or slightly wide
LPFB pattern
- RAD
- rS in I / aVL
- qR in II / III / aVF
- QRS usually normal
Is RBBB also present?
QRS ≥120 ms, rsR′ in V1, broad S in I / V6
Bifascicular block
RBBB + LAFB = most common
RBBB + LPFB = less common
RBBB + LPFB = less common
Isolated fascicular block
Isolated LAFB or isolated LPFB
PR >200 ms?
Trifascicular pattern
Bifascicular block + 1° AV block
Bifascicular block only
Pocket Guide
| Type | EKG Features | Notes |
|---|---|---|
| LAFB | LAD, qR in aVL, rS in II/III/aVF | Common, often benign |
| LPFB | RAD, rS in I/aVL, qR in II/III/aVF | Rare, usually structural disease |
| Bifascicular (RBBB + LAFB) | RBBB + LAD pattern | Most common bifascicular combo |
| Bifascicular (RBBB + LPFB) | RBBB + RAD pattern | Less common, consider ischemia |
| Trifascicular | Bifascicular + 1° AV block (PR >200 ms) | May progress to complete block |
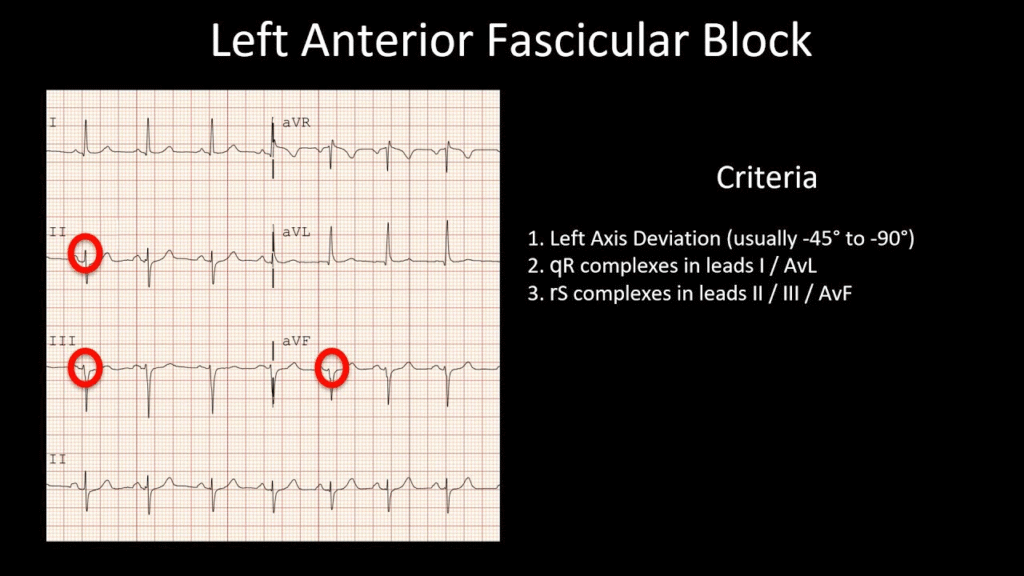
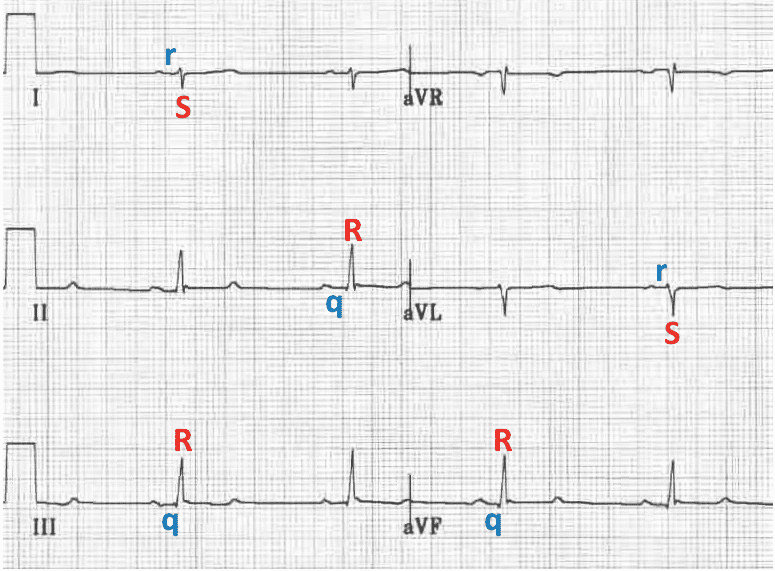
Left Anterior Fascicular Block (LAFB)
- Most common fascicular block
- EKG criteria:
- Left axis deviation (–45° to –90°)
- Small Q in leads I and aVL
- Small R in II, III, aVF
- Normal or slightly widened QRS (≤120ms)
- Often benign but may indicate underlying structural disease
Left Posterior Fascicular Block (LPFB)
- Rare (posterior fascicle is broader, dual supply)
- EKG criteria:
- Right axis deviation (>+90°) without other cause (RVH, PE)
- Small R in I and aVL, small Q in II, III, aVF
- Normal QRS duration
- Suspect structural heart disease
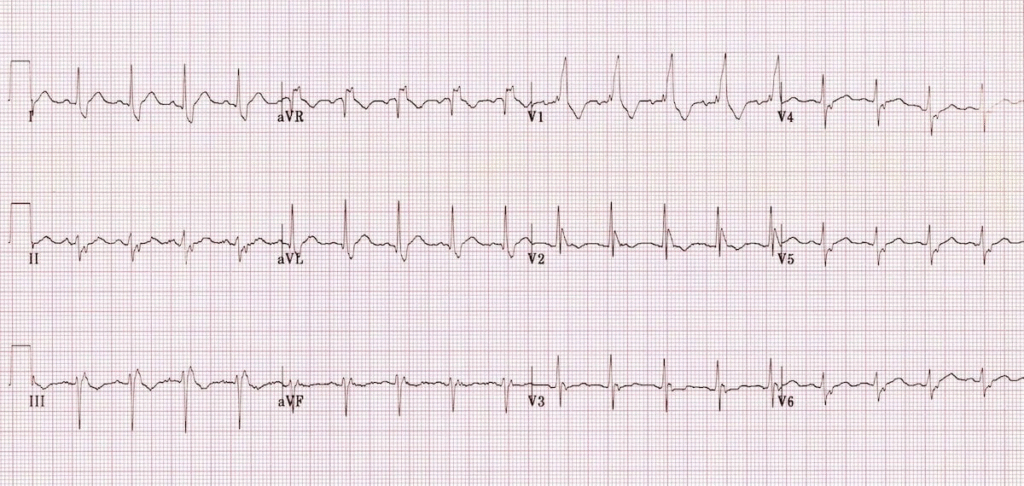
Bifascicular Block
- Involves any two of the three fascicles:
- RBBB + LAFB (most common)
- RBBB + LPFB
EKG
- RBBB: QRS ≥120 ms, rsR′ in V1, broad S in I/V6
- LAFB or LPFB criteria as above (in EKG below there is RBBB, LAD, normal QRS, rS complexes in inferior leads = RBBB + LAFB)
Clinical Significance
- Marker of conduction system disease
- Increases risk of progression to complete heart block, especially if:
- Alternating bundle branch block is present
- There's associated syncope
- May need pacemaker if symptomatic
Trifascicular Block
- Imprecise term; often refers to:
- RBBB + LAFB/LPFB + prolonged PR interval
- Not necessarily all 3 fascicles blocked simultaneously
- Consider EP study or pacing if symptomatic