
ECMO Troubleshooter
Pick VA vs. VV ECMO and bedside issue to see what it means, what to check now, and common fixes
What it usually means
Likely causes
Check now
How to fix it
Escalate / consider
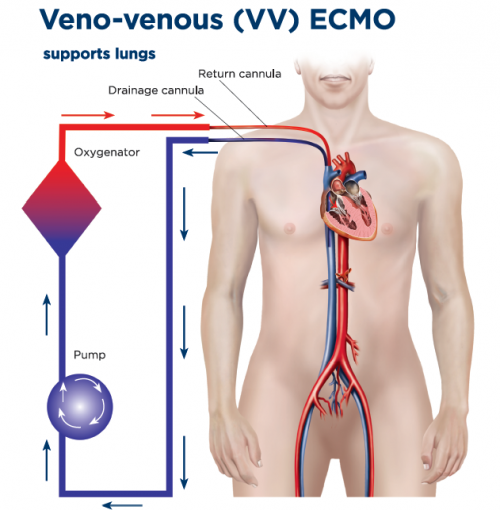
When to choose VV ECMO?
- Severe, potentially reversible respiratory failure (ARDS) refractory to optimal management
- Hypoxemia or hypercapnia despite lung-protective ventilation, proning, paralysis, or inhaled vasodilator
- Intact or manageable hemodynamics without need for circulatory support
- Typical setup: femoral–IJ or dual-lumen cannulation
- Targets: SaO₂ > 88–92%
- Goal: Rest the lung
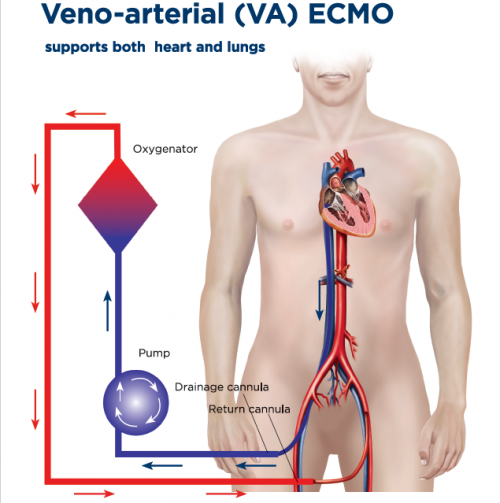
When to choose VA ECMO?
- Cardiogenic shock or cardiac arrest with potential for recovery or bridge
- Severe biventricular failure or refractory VT/VF, post-cardiotomy shock
- Need for hemodynamic support (MAP/perfusion) beyond vasoactives
- Typical setup: femoral VA
- Watch for: LV distension, Harlequin (north–south) syndrome
- Adjuncts: vent, Impella, or IABP if needed
Contraindications
- Irreversible disease without bridge or exit plan
- Multi-organ failure without recovery path
- Prohibitive bleeding/coagulopathy, devastating neuro injury
- Prolonged no-flow/low-flow arrest, advanced frailty, or poor baseline
Initial setup & targets
VV ECMO (oxygenation/CO₂)
- Blood flow ~5 L/min (up to 7–8). Aim > 60–70% of CO for SpO₂ > 90%
- Sweep 2–3 L/min, titrate to pCO₂
- Vent: tidal 3–4 mL/kg IBW, Pplat ≤ 25, PEEP individualized, FiO₂ minimal
- Goals: SpO₂ 88–92% (ok 85–88% if perfusion OK), pH > 7.25
Pearl: if sats low, check recirculation → flow → Hb/SaO₂/oxygenator
VA ECMO (perfusion/oxygenation)
- Flow titrated to MAP and end-organ perfusion. Treat LV distension early
- Monitor right radial ABG for Harlequin syndrome; add vent or V-A-V if needed
- Minimize catecholamines; optimize preload/afterload; unload LV if required
Anticoagulation
Heparin
- UFH unless bleeding risk → low-dose or no-anticoagulation strategy
- Anti-Xa preferred; aPTT/ACT adjunctive
- Anti-Xa: 0.3–0.7 IU/mL
- aPTT: 50–70 s
- ACT: 160–180 s
- Platelets: > 75–100 K
- Fibrinogen: > 150–200 mg/dL
Reassess after circuit change, bleeding, or oxygenator dysfunction.
ECMO Troubleshooting
| Problem | Likely Causes | Key Actions |
|---|---|---|
| Low SpO₂ (VV ECMO) | • Recirculation (cannula malposition) • Inadequate blood flow • Hypovolemia • Oxygenator dysfunction | • Check cannula position and flows • Increase blood flow • Optimize preload (volume) • Inspect oxygenator ΔP and color change • Reduce patient O₂ demand (sedation, temp) |
| Hypercapnia | • Inadequate sweep • Gas line obstruction • Oxygenator failure | • Increase sweep gas flow • Check gas line and blender • Minimize ventilator dead space • Replace oxygenator if unresponsive |
| Hypotension | • VV: vasodilation or low preload • VA: LV distension, tamponade, RV failure, sepsis, bleeding | • VV: give volume, titrate vasopressors • VA: evaluate with echo • Unload LV (IABP/Impella), treat underlying cause |
| Drainage insufficiency | • Hypovolemia • Cannula malposition • Obstruction or collapse of drainage line | • Trend circuit pressures • Lower head, give volume • Reduce pump RPM • Reposition or flush cannula |
| Return obstruction / Oxygenator failure | • Thrombus formation • High pre- to post-oxygenator ΔP • Oxygenator clot burden | • Inspect oxygenator visually • Check ΔP and post-membrane gases • Exchange circuit/oxygenator if needed |
| North–South (Harlequin) syndrome (VA ECMO) | • Differential oxygenation (native LV ejecting deoxygenated blood) | • Monitor right radial ABG • Increase ECMO flow and O₂ delivery • Add vent or convert to V-A-V configuration |
Weaning
VV ECMO
- Improving lung mechanics/oxygenation, minimal sweep
- Sweep-down or clamp test with permissive targets
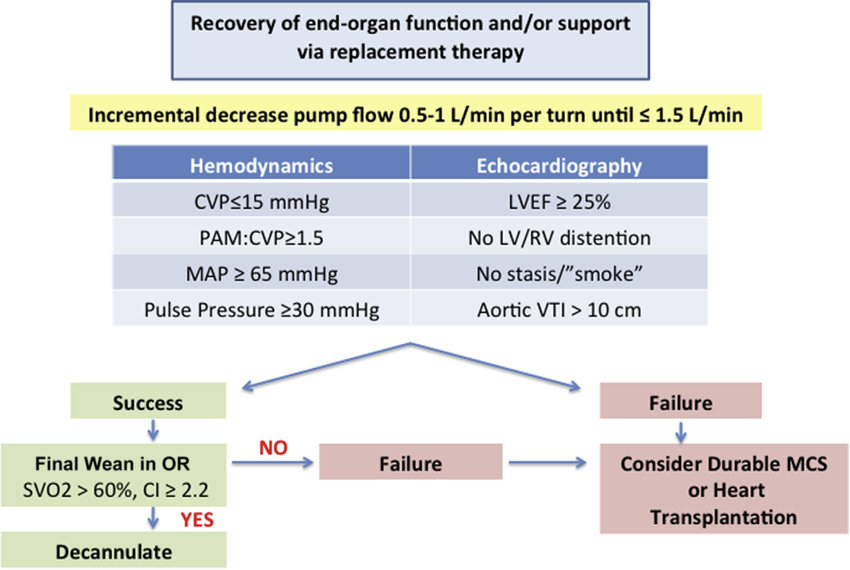
VA ECMO
- Recovery of native CO: increasing pulse pressure, less inotrope, improving echo (LVOT VTI, aortic valve opening)
- Stepwise flow reduction under echo and hemodynamic monitoring
Daily checklist
- Indication still valid; exit strategy defined
- Flows, sweep, vent targets documented
- Anticoagulation and labs in range; hemolysis markers trended
- Limb/neuro checks, cannula inspection, circuit visual check
- Echo/ultrasound as needed for recirculation, function, effusions