VT Localizer
Cheat Sheet
| Finding | Suggests |
|---|---|
| LBBB VT | RV origin |
| RBBB VT | LV origin |
| Inferior axis | Outflow tract or superior origin |
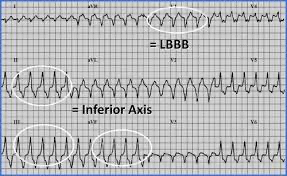
| LBBB + inferior axis | Classic RVOT VT pattern |
| High MDI | Epicardial VT |
| Structural abnormalities or scar | Idiopathic VT less likely |
RV or LV
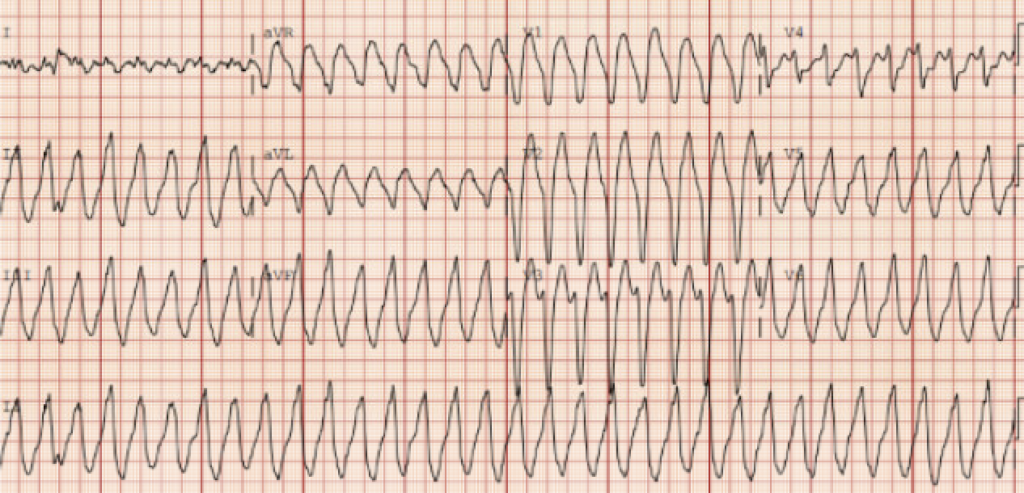
LBBB morphology
- Mostly negative in V1
- Usually means VT starts in the RV
- Reason: activation moves right to left
- Examples
- RVOT VT
- Other RV free wall VT
- ARVC-related VT
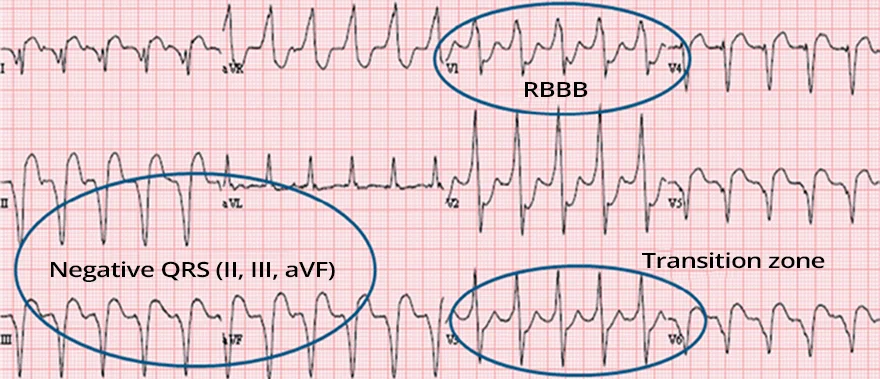
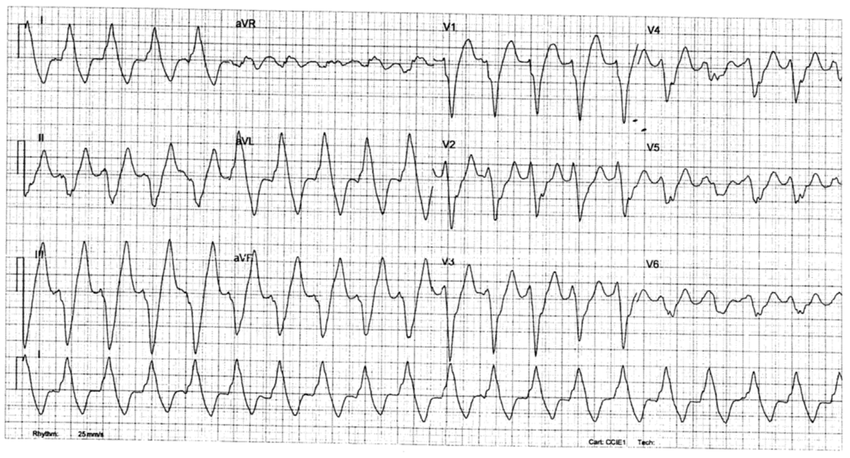
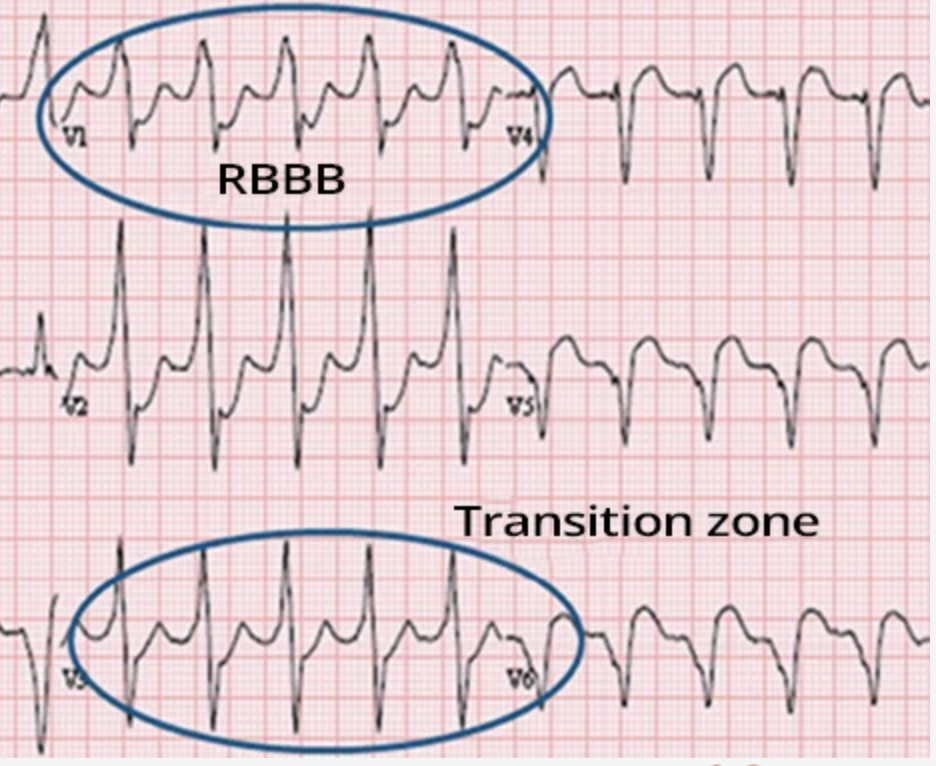
RBBB morphology
- Mostly positive in V1
- Usually means VT starts in the LV
- Reason: activation moves left to right
- Examples
- LV scar VT
- Fascicular VT
- LV summit / LVOT VT
Axis
Inferior axis
- Positive in II, III, aVF
- Impulse is traveling downward
- Suggests a superior origin
- Examples
- RVOT VT
- LVOT VT
Superior axis
- Negative in II, III, aVF
- Impulse is traveling upward
- Suggests an inferior origin
- Examples
- Inferior scar VT
- Apical or inferior ventricular origin
Precordial Transition
Late Transition
- More rightward / later transition can support RVOT origin
- Transition ≥ V5
Early Transition
- Earlier transition can support LVOT origin
- Transition in V1-V3
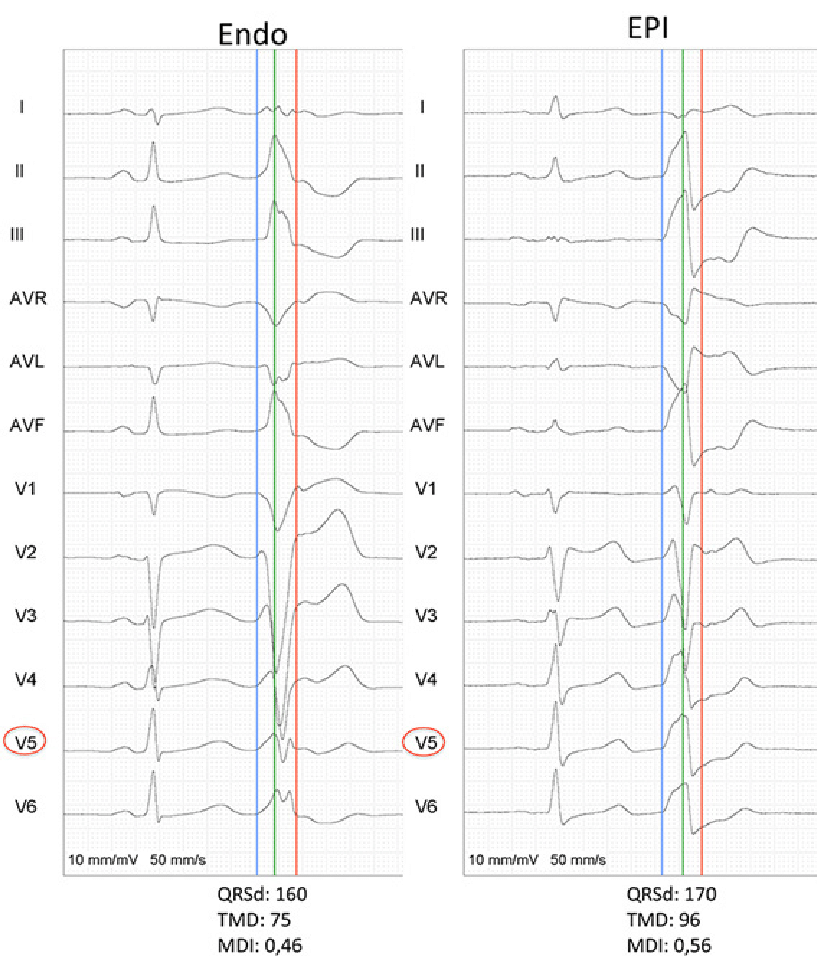
Maximum Deflection Index (MDI)
MDI helps predict epicardial vs endocardial origin
- MDI = time from QRS onset to maximum deflection / total QRS duration
- Helps plan epicardial (riskier) vs endocardial ablation
- Helps determine what disease process may be causing scar
- Pick a precordial lead with a clear VT complex
- Mark QRS onset
- Mark the point of maximum positive or negative deflection
- Measure: onset to maximum deflection and total QRS duration
- Divide the first by the second
- Interpretation
- MDI < 0.55: endocardial origin more likely
- MDI ≥ 0.55 to 0.60: epicardial origin more likely