
Asthma Control Test
Score 5-25. Higher score = better control.
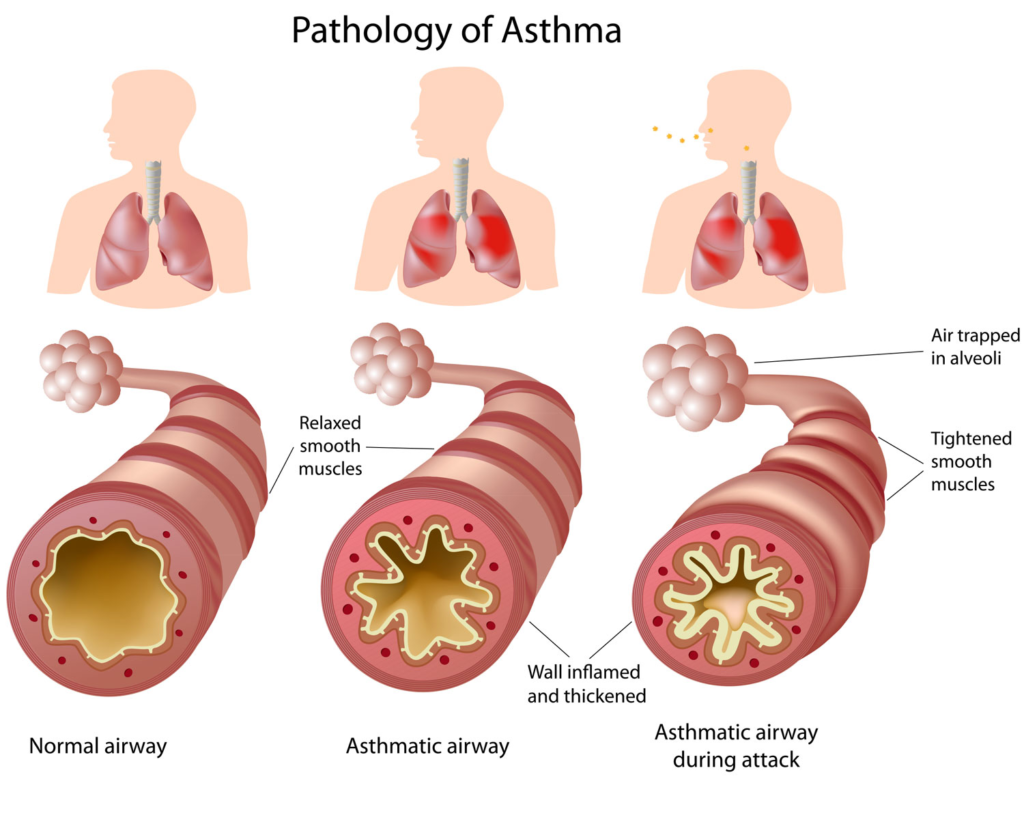
Symptoms/ Diagnosis
- Variable wheeze, cough, chest tightness, dyspnea
- Triggers: dust, pollen, smoke, wildfires, exercise, viral illness
- Ask about childhood asthma, family history, premature birth
- Spirometry with bronchodilator reversibility is standard
- FEV1 ↑ ≥12% and ≥200 mL supports asthma
- If spirometry normal → methacholine challenge
- PEF can assist if spirometry unavailable
PFT's
| Test | Findings in Asthma | Notes |
|---|---|---|
| FEV1/FVC Ratio | ↓ (Reduced) (<0.75-0.80) | Hallmark of obstructive lung disease |
| FEV1 (Post-Bronchodilator) | ↑ by ≥12% and ≥200 mL improvement | Confirms reversible airway obstruction |
| FEF 25-75% | ↓ (Reduced) | Suggests early small airway involvement |
| TLC (Total Lung Capacity) | Normal or ↑ | Hyperinflation may occur in severe cases |
| RV (Residual Volume) | ↑ (Increased) | Air trapping due to airway obstruction |
| DLCO (Diffusion Capacity) | Normal | Differentiates from COPD (which may have ↓ DLCO) |
| Methacholine Challenge | FEV1 ↓ by ≥20% at low doses | Indicates airway hyperreactivity when spirometry is normal |
Control
Asthma control is assessed using the Asthma Control Test (ACT)
- ACT ≥20 = well controlled
- ACT ≤19 = not well controlled
Treatment: Formoterol + ICS (Symbicort)
- Mild: PRN Symbicort. 2 puffs prior to trigger
- More symptoms: Symbicort BID with additional doses PRN for symptom relief
- Formoterol preferred over salmeterol due to rapid onset (5-10 min vs 2 hours)
- If no ICS-formoterol: use ICS whenever SABA used
- Montelukast for allergic/exercise/ASA-sensitive asthma
- Always check inhaler technique
Treatment Options
| Qualifying criteria | Step 1Intermittent / very mild | Step 2Mild persistent | Step 3Moderate symptoms | Step 4More severe / frequent symptoms | |
|---|---|---|---|---|---|
| Who fits this step |
|
|
|
|
|
| Option 1 | ICS-formoterol regimen | Low-dose ICS-formoterol as needed | Low-dose ICS-formoterol as needed | Low-dose ICS-formoterol maintenance + reliever | Medium-dose ICS-formoterol maintenance + reliever |
| Option 2 | Alternative maintenance | No daily controller |
Anti-inflammatory reliever only
or
Low-dose ICS daily
|
Low-dose ICS-LABA
or
Low-dose ICS + LAMA or LTRA
|
Medium-dose ICS-LABA
or
Medium-dose ICS + LAMA or LTRA
|
| and | and | and | and | and | |
| Alternative reliever |
ICS-SABA as needed
or
ICS + SABA as needed
or
SABA as needed
|
ICS-SABA as needed
or
ICS + SABA as needed
or
SABA as needed
|
ICS-SABA as needed
or
ICS + SABA as needed
or
SABA as needed
|
ICS-SABA as needed
or
ICS + SABA as needed
or
SABA as needed
|
Inpatient Management
- Assess severity: WOB, speech, accessory use, AMS, O2 need; red flags = silent chest, fatigue, rising CO2
- O2 to SpO2 >92%
- Bronchodilators: albuterol ± ipratropium (q2–4h or continuous if severe)
- Steroids early: IV or PO, do not delay
- Mg sulfate IV if severe or poor response
- Reassess frequently: WOB, air movement, SpO2
- VBG/ABG if worsening or c/f hypercapnia
- CXR only if atypical or c/f PNA/PTX
- Escalate: continuous nebs, consider NIV briefly, early ICU
- Intubate if AMS, exhaustion, rising CO2, refractory hypoxemia
- Avoid: sedatives, routine abx, stopping controller therapy
- Discharge: stable on spaced nebs, off O2, steroids completed/prescribed, on ICS regimen, inhaler teaching + follow-up
Assess asthma exacerbation severity
↓
Signs of impending respiratory failure?
No
↓
Severe exacerbation?
(PEF ≤50% predicted or personal best)
(PEF ≤50% predicted or personal best)
Yes
↓
Admit, ICU/Anesthesia consult
• SABA + ipratropium neb
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg
• IV magnesium sulfate 2 g over 20 min
• Assess alternate dx/comorbidities
• SABA + ipratropium neb
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg
• IV magnesium sulfate 2 g over 20 min
• Assess alternate dx/comorbidities
Severe exacerbation
↓
• Nebulized SABA or SABA/ipratropium q20 min x1 hr or continuous
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg
• Or prednisone 60 mg PO
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg
• Or prednisone 60 mg PO
Mild to moderate exacerbation
↓
• SABA by neb or MDI q20 min x1 hr, then PRN
• O2 target SpO2 >92%
• Prednisone 40 mg PO
• O2 target SpO2 >92%
• Prednisone 40 mg PO
Worsening
symptoms, PEF, SpO2
symptoms, PEF, SpO2
↓
Admit, ICU/Anesthesia consult
• SABA/ipratropium nebs
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg if not already given
• Assess alternate dx/comorbidities
• SABA/ipratropium nebs
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg if not already given
• Assess alternate dx/comorbidities
Good response
Symptoms resolved, PEF >80%
Symptoms resolved, PEF >80%
↓
Discharge home
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
Incomplete response
Persistent dyspnea/wheeze or PEF 60 to 80%
Persistent dyspnea/wheeze or PEF 60 to 80%
↓
Continue observed treatment for another 1 to 3 hours and reassess
Good response
Symptoms resolved, PEF >80%
Symptoms resolved, PEF >80%
↓
Discharge home
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
Incomplete response after reassessment
Persistent symptoms/wheeze or PEF 60 to 80%
Persistent symptoms/wheeze or PEF 60 to 80%
↓
Worsening
symptoms, PEF, SpO2
symptoms, PEF, SpO2
↓
Admit, ICU/Anesthesia consult
• SABA/ipratropium nebs
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg if not already given
• Assess alternate dx/comorbidities
• SABA/ipratropium nebs
• O2 target SpO2 93 to 95%
• IV methylprednisolone 40 to 60 mg if not already given
• Assess alternate dx/comorbidities
Still incomplete
PEF 60 to 80%, prior severe exacerbations, or poor adherence
PEF 60 to 80%, prior severe exacerbations, or poor adherence
↓
Admit to hospital
Continued treatment and monitoring
Continued treatment and monitoring
Substantial improvement
PEF 60 to 80%, good understanding/follow-up
PEF 60 to 80%, good understanding/follow-up
↓
Discharge home
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
• Reliever q4 to 6h PRN
• Prednisone 40 to 60 mg/day x 5 days
• Inhaler teaching + action plan
• PCP follow-up
• Resume/initiate ICS if needed
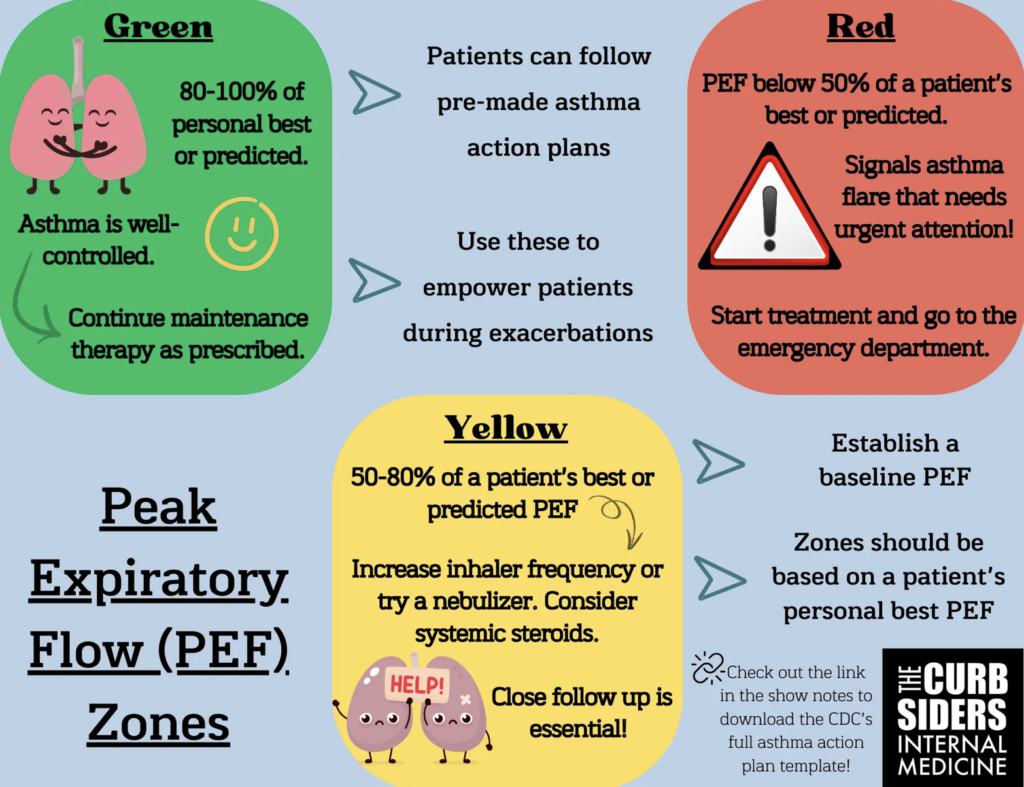
Outpatient Exacerbations
- Use personal best PEF
- Green ≥80% → continue usual meds
- Yellow 50–79% → step up meds, monitor closely
- Red <50% → send to ED
- Send to ED regardless of PEF if patient has: severe dyspnea, speaking only short phrases, accessory muscle use, no improvement after rescue therapy
Asthma Phenotypes
- High T2 Inflammation: Allergic asthma, high eosinophils, responds to ICS and biologics
- Low T2 Asthma: Poor response to biologics, limited treatment options
- Cough-variant Asthma: Montelukast may help
- Obesity-associated Asthma: Unique pathophysiology, often harder to control