
| Antiarrhythmic Drugs | |||||||
|---|---|---|---|---|---|---|---|
| Mechanism | Effect on Action Potential | Examples | Additional Actions | Side Effects | Indications | ||
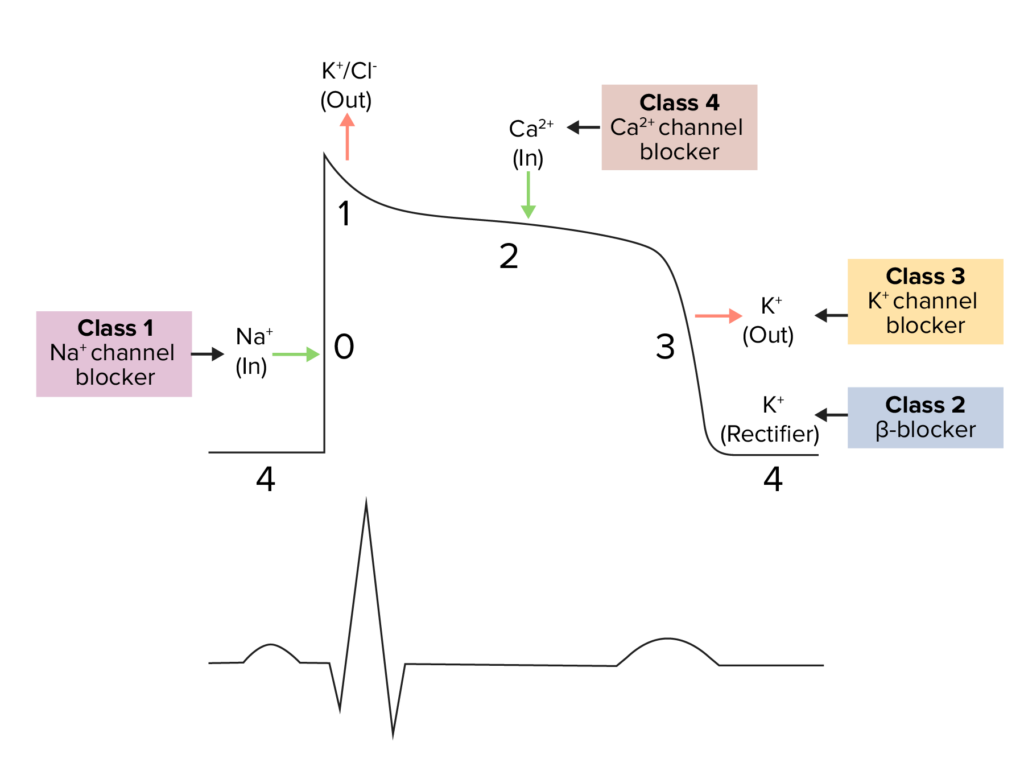
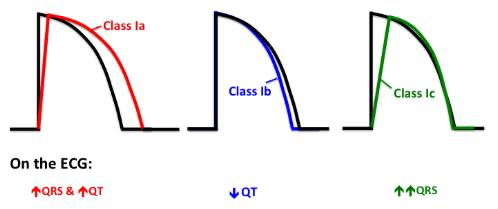
| I | Ia | Na+ channel blocker | ↓↓ upstroke rate ↑ AP duration |
Quinidine Procainamide | Class III activity |
|
|
| Ib | ↓ upstroke rate ↓ AP duration |
Lidocaine Mexiletine | None |
|
|
||
| Ic | ↓↓↓ upstroke rate Ø AP duration |
Propafenone Flecainide |
Class II activity (propafenone only) |
|
|
||
| II | β blocker | Slows rate of depolarization in slow AP cells | Metoprolol Esmolol Acebutolol Pindolol |
None |
|
|
|
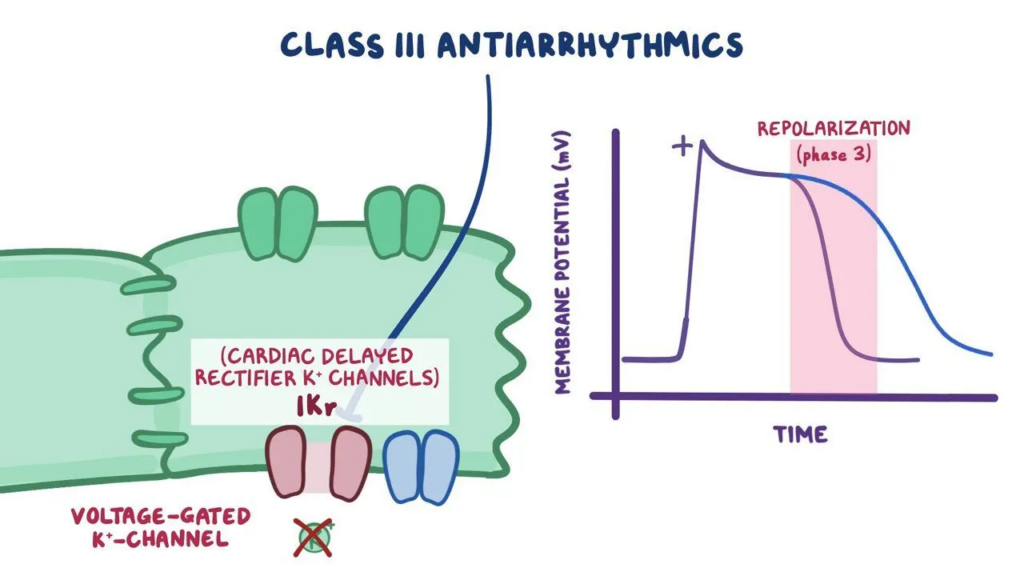
| III | K+ channel blocker | ↑↑↑ AP duration | Amiodarone | Class I, II, and IV activity |
|
|
|
| Dronedarone | Class I, II, and IV activity |
|
|
||||
| Sotalol | Class II activity |
|
|
||||
| Dofetilide | None |
|
|
||||
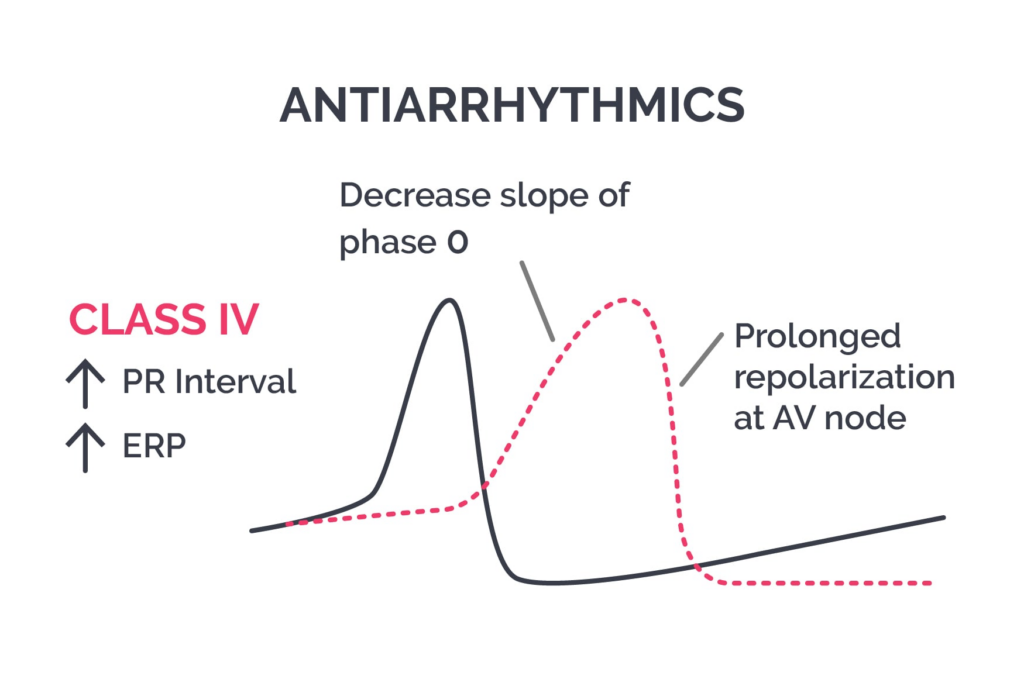
| IV | Ca2+ channel blocker | Slows rate of depolarization in slow AP cells | Verapamil Diltiazem | Vasodilation |
|
|
|
| Digoxin | ↑ vagal tone, inhibits Na+/K+ pump | Slows rate of depolarization in slow AP cells | N/A | Strengthens myocardial contraction |
|
|
|
| Adenosine | Induces AV block |
↑ refractory period ↑ threshold potential ↓ upstroke rate |
N/A | Vasodilation |
|
|
|
What's the physiology?
- What is the rhythm?
- AF / flutter
- AVNRT / AVRT
- Atrial tachycardia
- Monomorphic VT (scar)
- Polymorphic VT / torsades
- What is the substrate?
- Prior MI / scar
- LV dysfunction
- LVH
- Cardiomyopathy
- Channelopathies (LQT, Brugada)
- CKD / liver disease
- Conduction disease
- What is driving this right now?
- Sepsis
- Hypoxia
- Ischemia
- Electrolytes
- Volume status
Most antiarrhythmics can worsen the arrhythmia you are trying to treat.
Class I – Sodium Channel Blockers
Ia (procainamide, quinidine, disopyramide)
- Use:
- Procainamide
- Afib/AFlutter
- Stable VT
- Quinidine
- ****
- Procainamide
- Contraindications
- Infranodal conduction disease → progress to CHB
- Prolonged QT
- History of Torsades
- Uncorrected hypokalemia or hypomagnesemia
- QT prolongation → torsades
- Severe heart failure/hypotension → negative isotropy
- Side effects
- Hypotension, reduced CO
- Torsades
- Unique
- Procainamide → lupus
- Quinidine → myasthenia gravis
- Disopyramide → anticholinergic/ myasthenia
Ib (lidocaine, mexiletine)
- Use:
- Ventricular arrhythmias only
- Best in ischemia-related VT/VF
- Key concept (EMCrit):
- Lidocaine works best in acute ischemic myocardium
- Often does NOT terminate scar-mediated monomorphic VT
- Mexiletine:
- Oral lidocaine equivalent
- Adjunct, not strong monotherapy
- Side effects:
- Neurotoxicity
Ic (flecainide, propafenone)
- Use:
- AF rhythm control
- Pill-in-pocket
- ONLY if:
- No structural heart disease
- Key risk:
- Post-MI → increased mortality (CAST)
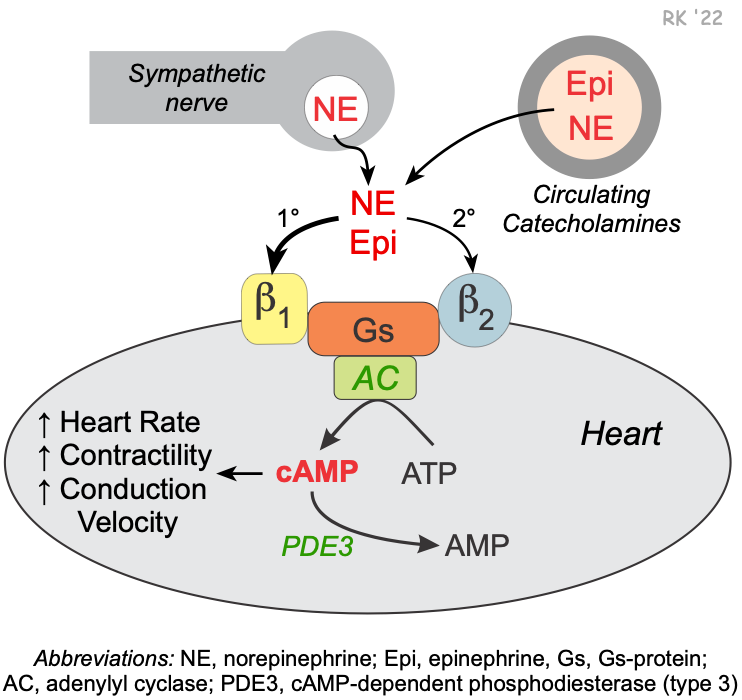
Class II – Beta-Blockers
- Use:
- AF rate control
- SVT
- VT suppression
- Long QT / CPVT
- High-yield:
- Often first-line safest antiarrhythmic
- Side effects:
- Bradycardia
- AV block
- Bronchospasm
Class III – Potassium Channel Blockers
Amiodarone
- Use:
- AF (especially structural disease / HFrEF)
- VT/VF
- Strength:
- Works in almost anything
- Weakness:
- Toxicity:
- Lung
- Thyroid
- Liver
- Toxicity:
Dofetilide
- Use:
- AF / flutter only
- Safe in HFrEF
- Must:
- Start inpatient
- Risk:
- Torsades
Sotalol
- Use:
- AF prevention
- VT suppression
- Avoid:
- CKD
- QT prolongation
Dronedarone
- Use:
- Select AF patients
- Avoid:
- Permanent AF
- HF (especially unstable)
Ibutilide
- Use:
- Chemical cardioversion (flutter > AF)
- Risk:
- Torsades
Class IV – Diltiazem, Verapamil
- Use:
- AF rate control
- SVT
- Avoid:
- HFrEF
- Pre-excited AF
Other Drugs
Adenosine
- Use:
- AVNRT / AVRT
- Diagnostic
- Avoid:
- Asthma
- Irregular wide-complex tachycardia
Digoxin
- Use:
- AF rate control (adjunct, especially HF)
- Weakness:
- Not effective for active patients
- Risk:
- Toxicity with renal dysfunction
AF / Flutter
Rate Control
- Beta-blocker
- Diltiazem / verapamil
- Digoxin (adjunct)
Rhythm Control
- No structural heart disease
- Flecainide
- Propafenone
- Dronedarone
- Sotalol
- Dofetilide
- Structural disease/ HFrEF
- Amiodarone
- Dofetilide
Ventricular Arrhythmias
Monomorphic VT (scar-mediated)
- Amiodarone
- Procainamide
- Sotalol
- Beta-blocker
- Mexiletine (adjunct)
- Lidocaine typically least effective if VT scar=mediated
Ischemic VT/VF
- Lidocaine is most useful here
- Amiodarone
- Beta-blocker
VT Storm
- Treat cause first:
- Ischemia
- Electrolytes
- Sympathetic surge
- Then:
- Beta-blockade + amio
- Sedation
Electrical Risk
Low-risk patients
- Hemodynamically stable VA
- Functioning ICD
- VA terminated by ATP
- Limited number of episodes
- No prior AAD therapy
Step 1: initial therapies
- Oral beta-blocker (eg propranolol)
- Amiodarone IV ± oral loading
- Benzodiazepine
Recurrent arrhythmias
High-risk patients
- Hemodynamically unstable VA
- No functioning ICD
- VA not terminated by ATP
- Incessant arrhythmias
- Failure of AAD therapy
Step 2: add-on therapies
- IV beta-blocker (eg esmolol)
- Lidocaine IV
- Dexmedetomidine
Recurrent arrhythmias
Step 3: rescue therapies
- Stellate ganglion block
- IV procainamide
- General anesthesia
- Urgent ablation
Definitive therapy
- Catheter ablation
- Heart transplant/LVAD
- Palliative care
| Intensity | Antiarrhythmic Drugs | Adrenergic Blockade | Sedation/Anxiolysis | Hemodynamic Support |
|---|---|---|---|---|
| Step 1 |
Amiodarone IV
|
Oral beta-blocker
|
Benzodiazepine
|
Vasopressors
|
| Step 2 |
Lidocaine IV
|
IV beta-blocker
|
Dexmedetomidine
|
Intra-aortic balloon pump
|
| Step 3 |
Procainamide IV
|
Stellate ganglion blockade
|
General anesthesia
|
Advanced MCS
|
Torsades / Long QT
- Magnesium
- Stop offending drugs
- Overdrive pacing or isoproterenol
High-Yield Contraindications
- Flecainide / propafenone → structural disease
- Dronedarone → permanent AF, HF
- Dofetilide → QT prolongation, severe CKD
- Sotalol → CKD, QT
- Diltiazem / verapamil → HFrEF, pre-excited AF
- Adenosine → asthma, irregular wide complex
- Digoxin → renal failure, electrolyte issues