
Angina with Non-Obstructive Coronary Arteries
- ANOCA is common, underrecognized, and not benign
- It includes patients with angina despite non-obstructive coronary disease and often reflects coronary vasospasm, coronary microvascular dysfunction, myocardial bridging, or a combination of these mechanisms
- Women are disproportionately affected, but ANOCA occurs in both men and women
Why it matters
A large proportion of patients referred for coronary angiography for chronic angina are found to have non-obstructive CAD. ANOCA is associated with higher rates of major adverse cardiovascular events, all-cause mortality, reduced quality of life, repeat hospital visits, and substantial healthcare costs. It should not be dismissed as harmless chest pain.
Definitions
- MINOCA refers to myocardial infarction with non-obstructive coronary arteries
- INOCA refers to ischemia with non-obstructive coronary arteries
- ANOCA refers to angina with non-obstructive coronary arteries
Pathophysiology
ANOCA is not a single diagnosis. Common endotypes include:
- Coronary vasospasm
- Abnormal endothelial function can cause inappropriate epicardial or microvascular vasoconstriction, leading to angina, ischemic EKG changes, and recurrent symptoms.
- Coronary microvascular dysfunction
- Abnormal microvascular structure or function impairs coronary blood flow reserve and can produce ischemia even when epicardial arteries are not obstructed.
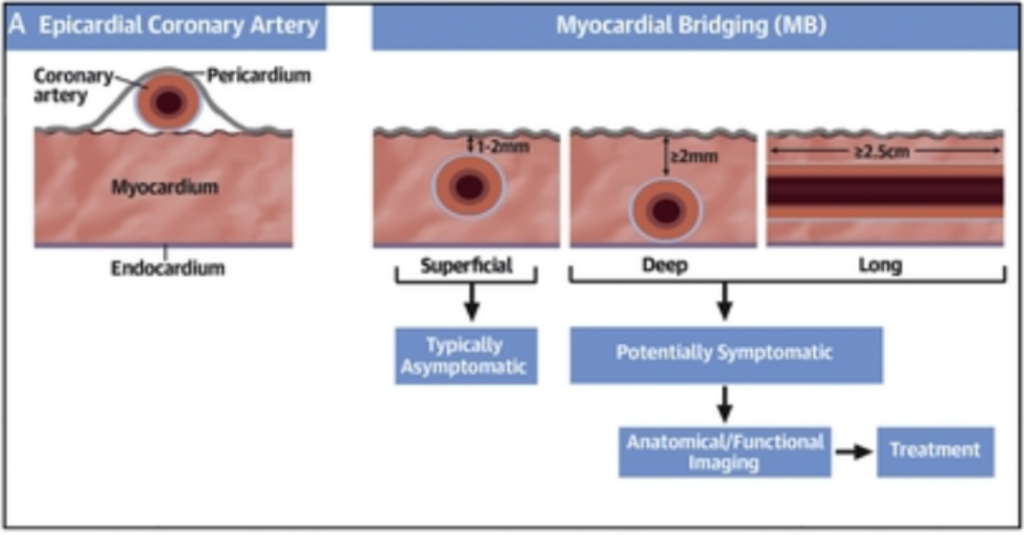
- Myocardial bridge
- A tunneled segment of coronary artery, usually in the LAD, can become hemodynamically significant and contribute to exertional angina or ischemia.
Clinical presentation
Patients typically report chest pain, pressure, or discomfort, often triggered by exertion or emotional stress, though symptoms can also occur at rest. Dyspnea is common. Many patients experience symptoms for years before diagnosis, are told their symptoms are non-cardiac, or are discharged without treatment despite recurrent presentations.
Prognosis and burden
ANOCA carries real morbidity. Compared with patients with normal coronaries, those with non-obstructive CAD have higher rates of MACE and death. Quality of life is often significantly impaired, with reduced exercise tolerance, effects on work and social life, and frequent repeat hospitalizations and angiography. Economic burden is also substantial.
Diagnostic evaluation
- Non-invasive testing
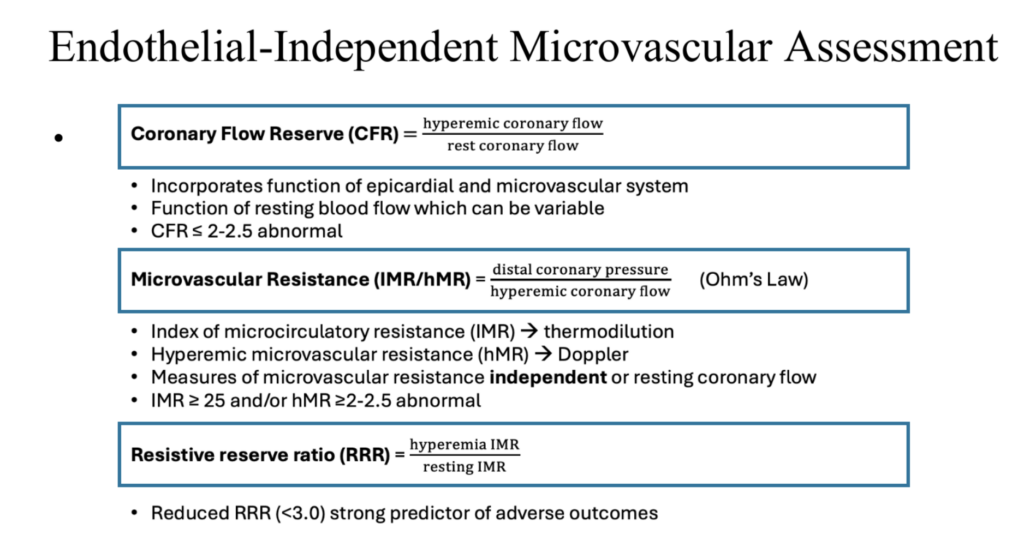
- Cardiac PET can assess coronary flow reserve and evaluate endothelial-independent microvascular dysfunction.
- Stress perfusion cardiac MRI can identify ischemia and reduced myocardial perfusion reserve.
- CCTA is useful for identifying myocardial bridge anatomy.
- Invasive testing
- Comprehensive invasive testing is the most complete diagnostic approach because it can assess:
- Epicardial coronary disease
- Endothelial-dependent dysfunction and vasospasm with acetylcholine
- Endothelial-independent microvascular dysfunction with adenosine-based CFR and IMR/hMR assessment
- Hemodynamic significance of myocardial bridge with physiologic testing
- Coronary angiography plus adjunctive coronary function testing identifies a mechanism in most patients with ANOCA.
Key endotypes
- Endothelial dysfunction
- Failure of normal epicardial vasodilation and coronary flow increase in response to acetylcholine.
- Microvascular spasm
- Angina and ischemic EKG changes without visible epicardial spasm.
- Epicardial coronary spasm
- Severe epicardial constriction with angina and ischemic EKG changes.
- Coronary microvascular dysfunction
- Reduced CFR and/or elevated IMR or hMR suggesting impaired microvascular vasodilator function.
Why coronary function testing matters
The CorMicA trial showed that invasive coronary function testing linked to stratified therapy improved angina, quality of life, illness perception, and treatment satisfaction. Benefits persisted at 6 and 12 months. This supports a precision-medicine approach rather than labeling these patients as having unexplained chest pain.
Guideline support
Both ACC/AHA and ESC guidelines support coronary function testing in appropriately selected patients with ANOCA or INOCA. PET and cardiac MRI also have a role, especially for non-invasive evaluation.
Management
Treatment depends on the endotype.
- Vasospasm
- Calcium channel blockers and nitrates are mainstay
- Coronary microvascular dysfunction
- Management focuses on mechanism-directed antianginal therapy plus aggressive treatment of cardiovascular risk factors.
- Myocardial bridge
- Beta blockade is often useful when bridge physiology is hemodynamically significant, while anatomy alone does not establish clinical importance.
IMR ≥25
no epicardial spasm
↓ flow with ACh
+ angina + EKG
dFFR ≤0.76