
Primary Read
Calculated Values
Mixed Disorder Check
Likely Causes to Consider
Suggested Next Steps
Initial Acid-Base Approach
Metabolic or respiratory?
- Metabolic = abnormal bicarb or anion gap
- Respiratory = abnormal pCO2
Check anion gap (AG = Na - Cl - HCO3)
- Normal AG: 4-12
- High AG → AGMA workup
- Normal AG + low bicarb → NAGMA
- High bicarb → metabolic alkalosis
If AG elevated, calculate delta-delta
- ΔAG = AG - 10
- ΔHCO3 = 24 - HCO3
- ΔAG ≈ ΔHCO3 → pure AGMA
- ΔAG > ΔHCO3 → AGMA + metabolic alkalosis
- ΔAG < ΔHCO3 → AGMA + NAGMA
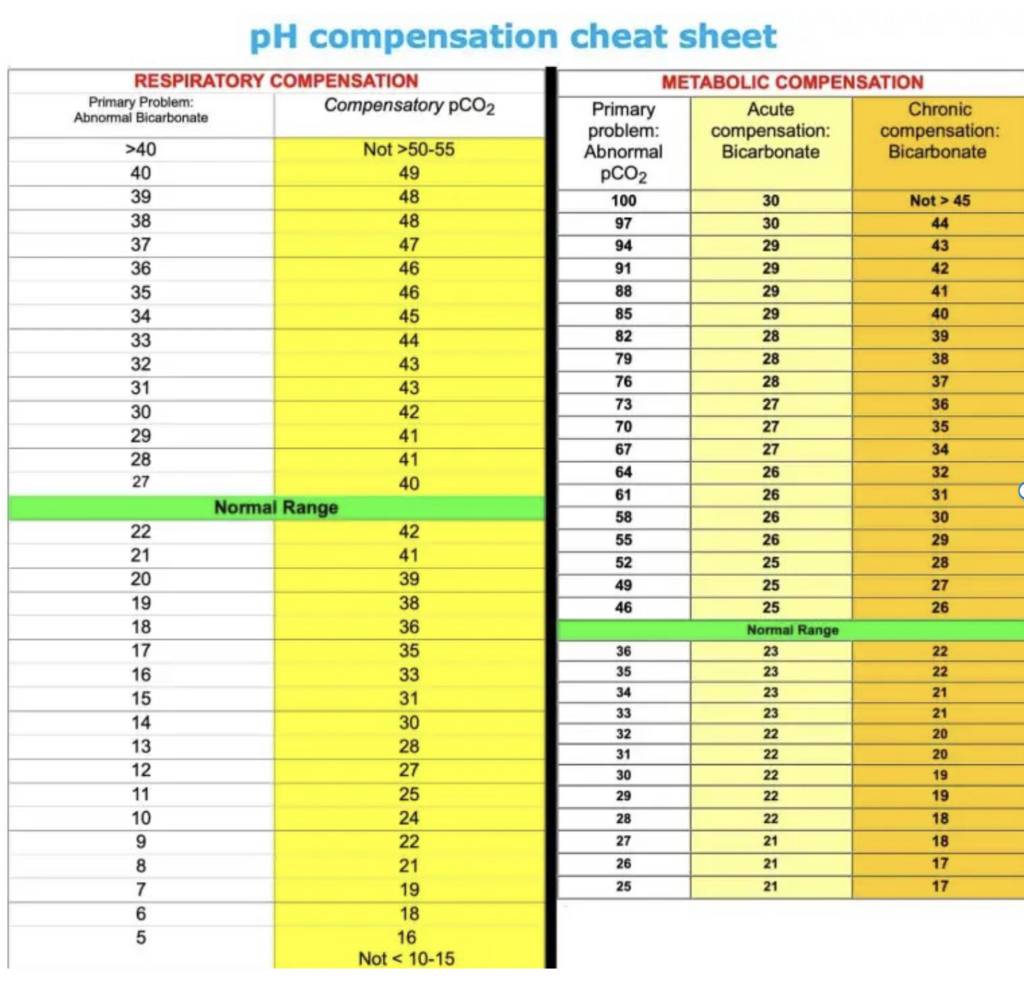
Evaluate respiratory compensation
- Use Winter’s formula: Expected pCO2 = (1.5 × HCO3) + 8 ±2
Ask:
- Is compensation appropriate?
- Is there another mixed disorder?
Compensation Cheat Sheet
Anion Gap Metabolic Acidosis (AGMA)
Common causes
- Lactic acidosis
- DKA/alcoholic/starvation ketoacidosis
- Renal failure/uremia
- Toxic alcohols
- Salicylates
- Acetaminophen toxicity
- Metformin
- Linezolid
- Propylene glycol
- Cyanide/CO poisoning
Lactic acidosis
- Inadequate oxygen delivery
- Shock
- Ischemia
- Seizure
- Severe anemia
- Adequate oxygen delivery
- Liver failure
- Malignancy
- Thiamine deficiency
- Beta agonists/epinephrine
- Severe DKA
Workup
- CBC
- CMP/Ca/Mg/Phos
- Lactate
- Beta-hydroxybutyrate
- LFTs
- Toxicology if indicated
- Medication review
- Calculate delta-delta
Exam
- Shock
- Poor perfusion
- Cold extremities
- Abdominal ischemia
- Altered mentation
Treatment
- Treat underlying cause
- IV thiamine 200mg q12h if unclear etiology/alcohol use/malnutrition
- Dialysis for severe renal failure or intoxications
- Bicarb mainly helpful in uremic acidosis
Dialysis indications
- pH <7.15 despite treatment
- Methanol
- Ethylene glycol
- Severe salicylate toxicity
- Severe metformin acidosis
Pearls
- Mild lactic acidosis can occur with normal AG
- Chronic CKD patients may have elevated baseline AG
- Beta-hydroxybutyrate better than urine ketones
Normal Anion Gap Metabolic Acidosis (NAGMA)
Causes
- Diarrhea
- Pancreatic/biliary losses
- Normal saline
- Resolving DKA
- Renal insufficiency
- RTA
- TPN
Potassium clues
High/normal K
- Type IV RTA
- CKD
- NS infusion
Low K
- GI losses
- Type I/II RTA
Workup
- CMP/Ca/Mg/Phos
- UA
- Urine electrolytes
- Urine pH
- Urine osmolar gap
Urine osmolar gap
= Urine osm - 2(Na + K) - glucose/18 - urea/28
Interpretation
- 150 → adequate ammonium excretion
- <150 → impaired ammonium excretion
Type IV RTA
Causes
- Diabetes
- ACEI/ARB
- NSAIDs
- Adrenal insufficiency
- Heparin
- Obstructive uropathy
- K-sparing diuretics
Treatment
- Treat underlying cause
- Fludrocortisone if appropriate
- Bicarb if:
- HCO3 <18
- AKI
- DKA
- clinically significant acidosis
Bicarbonate deficit = 0.4 × weight (kg) × (goal HCO₃ − current HCO₃)
Clinical correlation required. Severe acidemia generally requires treatment of the underlying cause first.
Volume-based treatment
Hypovolemic
- Give sodium bicarbonate
Euvolemic
- Add bicarbonate
- Remove chloride
Hypervolemic
- Diurese chloride
RTA's
RTA Predictor
Rule-based estimate of RTA type from common lab patterns
Use only after confirming non-anion gap metabolic acidosis. This does not replace clinical judgment.
Renal Tubular Acidosis Comparison
| RTA-1 Generalized distal |
RTA-2 Proximal |
RTA-4 Aldosterone resistance or deficiency |
|
|---|---|---|---|
| Lab findings | |||
| Typical severity of acidosis | Bicarb ~10–20 mM | Bicarb ~12–20 mM | Mild, bicarb >17 mM |
| Potassium | ↓↓ | ↓ | ↑ often primary manifestation |
| Other electrolytes | In generalized proximal tubule dysfunction: ↓ Ca, ↓ Mg, ↓ Phos, ↓ uric acid | ||
| Glucosuria | - | + | - |
| Urine pH | >5.3 | Variable | Usually <5.5 |
| Urine osmolar gap | <150 mOsm | >150 mOsm | <150 mOsm |
| Causes | |||
| Medications |
|
|
|
| Genetic disorders |
|
|
|
| Metabolic disorders |
|
|
|
| Other |
|
|
|
Metabolic Alkalosis
Common causes
Saline responsive
- Vomiting
- NG suction
- Contraction alkalosis
- Chloride wasting
Saline unresponsive
- Hyperaldosteronism
- HypoK/hypoMg
- Excess alkali
- Ongoing diuretics
Compensatory
- Chronic hypercapnia
- COPD
- OHS
Workup
- History/volume status
- Urine chloride
- Urine potassium
- ABG/VBG
Urine chloride interpretation
- <10-30 → saline responsive
- 10-30 → saline unresponsive
If persistent/refractory
Check renin/aldosterone
Interpretation
- ↓ renin, ↑ aldosterone → primary hyperaldo
- ↑ renin, ↑ aldosterone → secondary hyperaldo
- ↓ renin, ↓ aldosterone → apparent mineralocorticoid excess
When NOT to treat
- Chronic compensatory alkalosis from chronic hypercapnia
Treatment
- Replete K aggressively
- Replete Mg
- NS if hypovolemic
- Acetazolamide if hypervolemic
- Hold/reduce loop diuretics
- PPI if vomiting/NG suction
- Dialysis rarely needed
- IV HCl only as last resort
Respiratory Acidosis
Diagnosis
- pCO2 >45
- Determine acute vs chronic by bicarb level
Symptoms
- Somnolence
- Delirium
- Headache
- Asterixis
- CO2 narcosis
Causes
Won’t breathe
- Opioids
- Benzos
- Alcohol
- Brainstem pathology
- Hypothyroidism
Can’t breathe
- Neuromuscular disease
- Cervical cord injury
- MG/GBS/ALS
- Obesity hypoventilation
- Pleural effusion
- COPD/asthma
- Airway obstruction
Breathing ineffective
- Pneumonia
- ARDS
- PE
Workup
- Exam
- RR/mental status
- Neuro exam
- Lung exam
- CMP/CBC/TSH/CK
- CXR/CT/MRI as indicated
Treatment
- Treat underlying cause
- Naloxone for opioids
- NIV for neuromuscular weakness
- COPD/asthma-specific therapy
- Permissive hypercapnia often acceptable on vent
Pearls
- Chronic hypercapnia usually well tolerated
- Avoid rapid normalization in chronic retainers
Respiratory Alkalosis
Diagnosis
- pCO2 <35
Symptoms
- Anxiety
- Paresthesias
- Cramps
- Delirium
- Arrhythmias
Causes
Pulmonary
- PE
- Pneumonia
- Asthma
- Pneumothorax
CNS
- Pain
- Anxiety
- Stroke
- Meningitis
Medications
- Salicylates
- Caffeine
- Nicotine
- Beta agonists
- Progesterone
Other
- Pregnancy
- Thyrotoxicosis
- Cirrhosis
- Early sepsis
Workup
- Salicylate level
- TSH
- LFTs
- Beta-HCG
- PE evaluation
- Sepsis workup
Treatment
- Treat underlying cause
- Adequate pain control/sedation
- Reduce RR or TV if ventilated
References
- Adrogué, H. J., & Madias, N. E. (1998). Management of life-threatening acid-base disorders: First of two parts. The New England Journal of Medicine, 338(1), 26–34. https://doi.org/10.1056/NEJM199801013380106
- Adrogué, H. J., & Madias, N. E. (1998). Management of life-threatening acid-base disorders: Second of two parts. The New England Journal of Medicine, 338(2), 107–111. https://doi.org/10.1056/NEJM199801083380207
- Berend, K., de Vries, A. P. J., & Gans, R. O. B. (2014). Physiological approach to assessment of acid-base disturbances. The New England Journal of Medicine, 371(15), 1434–1445. https://doi.org/10.1056/NEJMra1003327
- Kraut, J. A., & Madias, N. E. (2010). Metabolic acidosis: Pathophysiology, diagnosis and management. Nature Reviews Nephrology, 6(5), 274–285. https://doi.org/10.1038/nrneph.2010.33
- Kraut, J. A., & Madias, N. E. (2012). Treatment of acute metabolic acidosis: A pathophysiologic approach. Nature Reviews Nephrology, 8(10), 589–601. https://doi.org/10.1038/nrneph.2012.186
- Kraut, J. A., & Kurtz, I. (2015). Treatment of acute non-anion gap metabolic acidosis. Clinical Kidney Journal, 8(1), 93–99. https://doi.org/10.1093/ckj/sfu126
- Palmer, B. F., Kelepouris, E., & Clegg, D. J. (2021). Renal tubular acidosis and management strategies: A narrative review. Advances in Therapy, 38(2), 949–968. https://doi.org/10.1007/s12325-020-01587-5
- Palmer, B. F., & Clegg, D. J. (2023). Respiratory acidosis and respiratory alkalosis: Core Curriculum 2023. American Journal of Kidney Diseases, 82(3), 347–359. https://doi.org/10.1053/j.ajkd.2023.02.004