
Atrial Flutter Type
Step 1
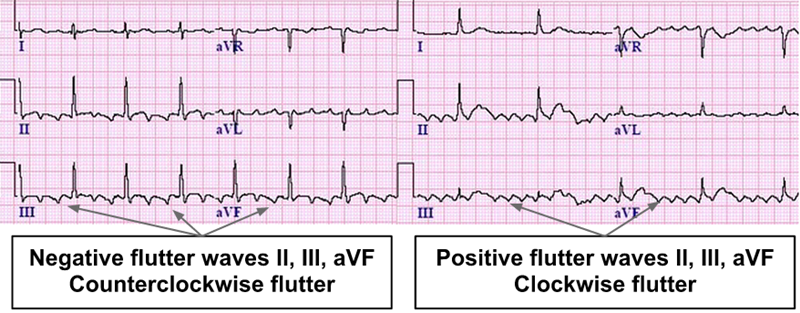
Are flutter waves negative in the inferior leads?
Look at II, III, and aVF.
Step 2
What is the flutter wave pattern in V1?
V1 helps estimate right vs left atrial activation.
Step 3
Is there an isoelectric baseline between flutter waves?
A clear isoelectric segment favors atypical flutter or focal atrial tachycardia.
Step 4
History of ablation, MAZE, valve surgery, congenital repair, or known atrial scar?
Scar strongly increases likelihood of atypical macroreentrant flutter.
Estimated Pattern
EKG Pearls
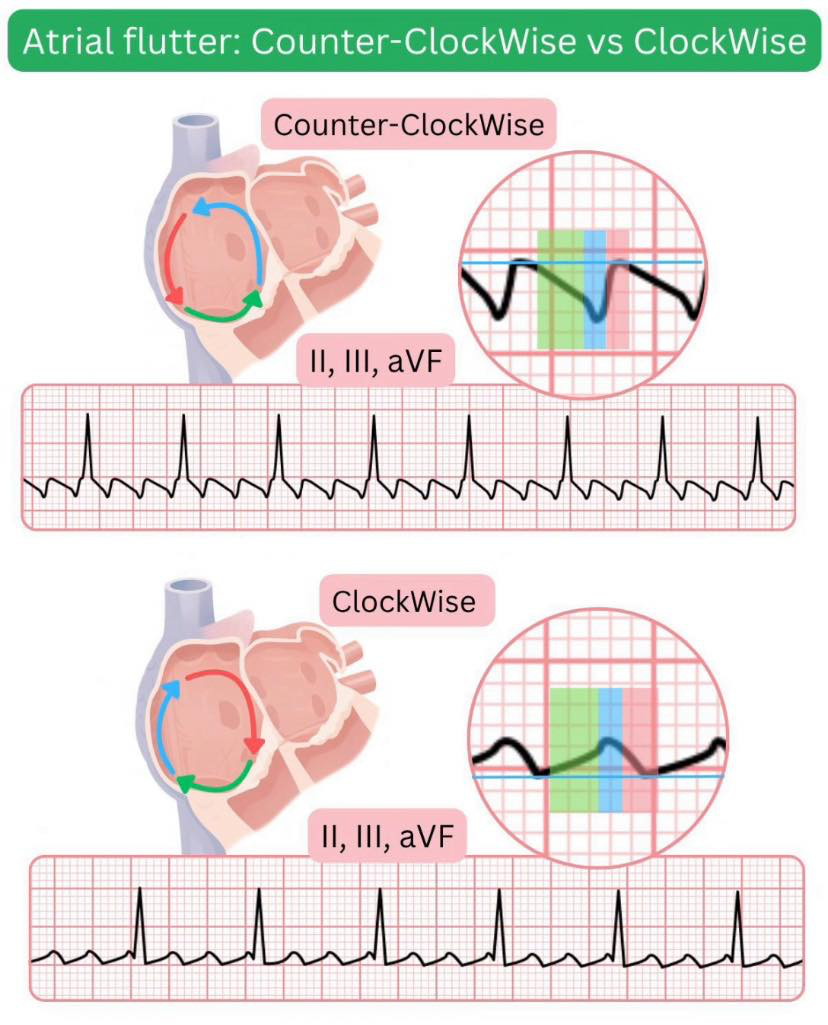
- Negative flutter waves in II, III, aVF with positive V1 favors typical counterclockwise CTI-dependent flutter.
- Positive inferior flutter waves with negative V1 favors reverse typical clockwise CTI-dependent flutter.
- Isoelectric baseline, unusual morphology, or prior atrial scar favors atypical flutter or macroreentrant atrial tachycardia.
- Surface EKG can suggest RA vs LA origin, but definitive localization usually requires EP mapping.
Core distinction
Typical flutter
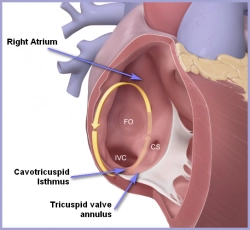
- Cavotricuspid isthmus (CTI) dependent
- Circuit around tricuspid annulus (RA)
Atypical flutter
- Not CTI dependent
- Often scar-related (RA or LA)
- Common after AF ablation or cardiac surgery
EKG clues
Typical (counterclockwise)
- Negative flutter waves in II, III, aVF
- Positive in V1
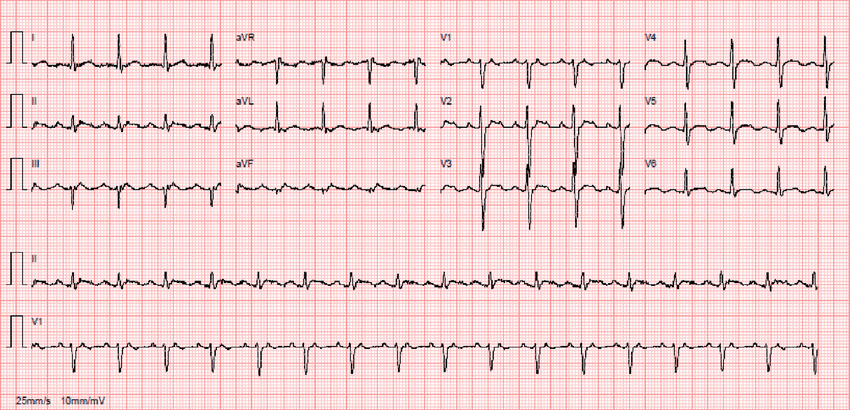
- Classic sawtooth pattern
- Atrial rate ~240–300
Reverse Typical (clockwise)
- Less common
- Often positive flutter waves in inferior leads
- Still CTI dependent
Atypical
- No classic sawtooth
- Variable or unusual flutter wave morphology
- Changing patterns across EKGs
- Often in patients with:
- Prior AF ablation
- Prior cardiac surgery
- Structural heart disease
Ablation implications
Typical flutter
- Target CTI line (RA)
- Standardized procedure
- High success
- Low recurrence
- Relatively quick
Atypical flutter
- Target depends on circuit
- Requires detailed mapping
- Often LA or scar-related
- Longer, more complex
- Lower success, higher recurrence
References
- Saoudi, N., Cosío, F., Waldo, A., Chen, S.-A., Iesaka, Y., Lesh, M., Saksena, S., Salerno, J., Schoels, W., & Working Group of Arrhythmias of the European Society of Cardiology. (2001). Classification of atrial flutter and regular atrial tachycardia according to electrophysiologic mechanism and anatomic bases: A statement from a joint expert group. European Heart Journal, 22(14), 1162–1182. https://doi.org/10.1053/euhj.2001.2658
- Cosío, F. G. (2017). Atrial flutter, typical and atypical: A review. Arrhythmia & Electrophysiology Review, 6(2), 55–62. https://doi.org/10.15420/aer.2017.5.2
- Page, R. L., Joglar, J. A., Caldwell, M. A., Calkins, H., Conti, J. B., Deal, B. J., Estes, N. A. M., III, Field, M. E., Goldberger, Z. D., Hammill, S. C., Indik, J. H., Lindsay, B. D., Olshansky, B., Russo, A. M., Shen, W.-K., Tracy, C. M., & Al-Khatib, S. M. (2016). 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. Journal of the American College of Cardiology, 67(13), e27–e115. https://doi.org/10.1016/j.jacc.2015.08.856
- Katritsis, D. G., Boriani, G., Cosio, F. G., Hindricks, G., Jais, P., Josephson, M. E., Keegan, R., Kim, Y.-H., Knight, B. P., Kuck, K.-H., Lane, D. A., Lip, G. Y. H., Malmborg, H., Oral, H., Pappone, C., & Themistoclakis, S. (2020). 2019 ESC guidelines for the management of patients with supraventricular tachycardia. European Heart Journal, 41(5), 655–720. https://doi.org/10.1093/eurheartj/ehz467
- Cosío, F. G., Arribas, F., López-Gil, M., Palacios, J., & Goicolea, A. (1996). Atrial flutter mapping and ablation. I. Studying atrial flutter mechanisms by mapping and entrainment. Pacing and Clinical Electrophysiology, 19(5), 841–853. https://doi.org/10.1111/j.1540-8159.1996.tb03348.x
- Calkins, H., Canby, R., Weiss, R., Taylor, G., Wells, P., Chinitz, L., Milstein, S., Compton, S., Oleson, K., Sherfesee, L., Onufer, J., & Badhwar, N. (2004). Results of catheter ablation of typical atrial flutter. American Journal of Cardiology, 94(4), 437–442. https://doi.org/10.1016/j.amjcard.2004.04.056