
IABP Troubleshooting Tool
Device / waveform issue
Clinical trajectory
Complications present
Bedside checks
Recommendation
Likely issue
Immediate actions
Check next
Disposition
Inflation
- Occurs in early diastole
- Raises aortic diastolic pressure
- Improves coronary perfusion
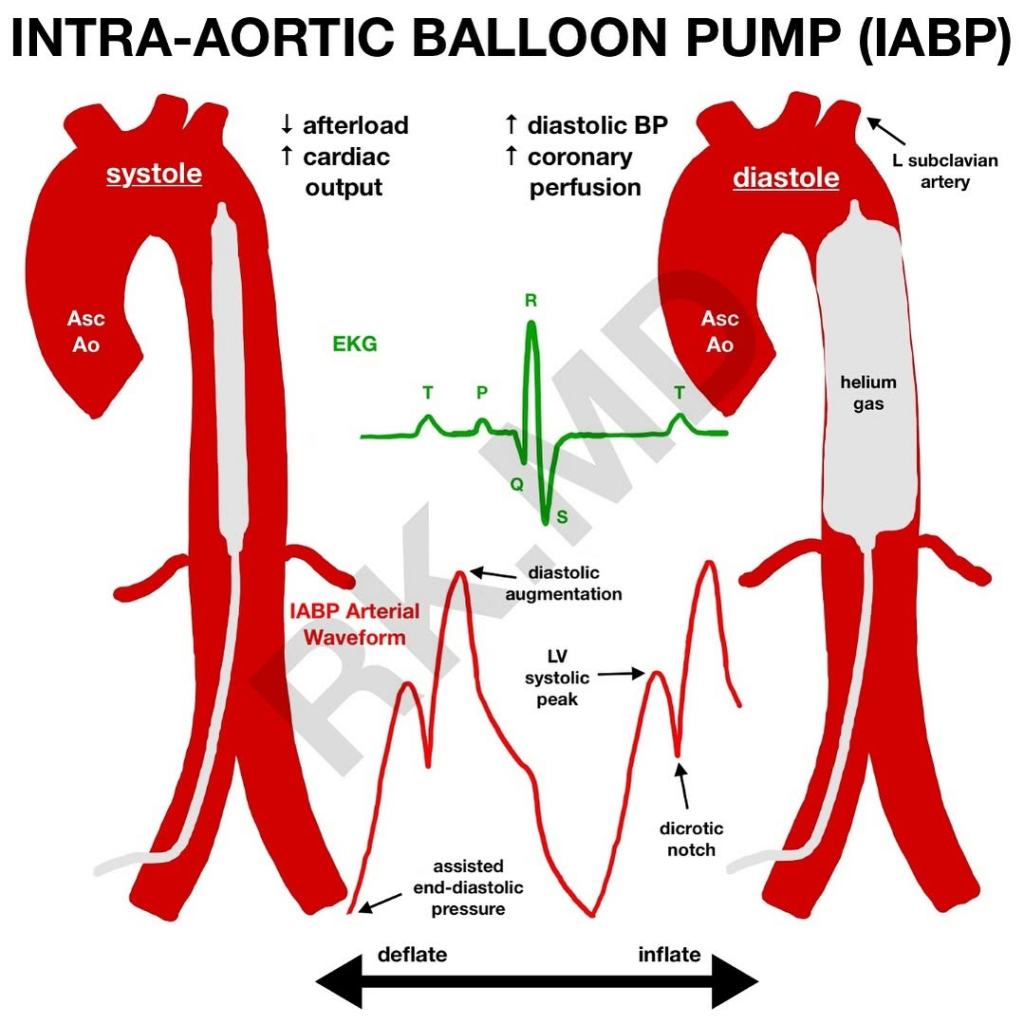
Deflation
- Occurs immediately before systole
- Lowers LV afterload
- Decreases LV wall stress and myocardial O2 demand
- May modestly improve cardiac output
Most useful when there is
- LV-predominant failure
- Active ischemia
- Need for modest LV unloading
- Mechanical complication of MI
- Bridge to PCI, CABG, valve surgery, recovery, escalation, or goals/decision
Common indications
- Refractory ischemia or unstable angina as bridge to revascularization
- Mechanical complications of MI:
- Acute MR from papillary muscle rupture
- Post-MI VSD
- Selected high-risk PCI
- Post-cardiotomy low output state
- Selected cardiogenic shock with active ischemia
- Selected acute decompensated HFrEF with low output
Contraindications
| Type | Contraindication | Why it matters |
|---|---|---|
| Absolute / major | Moderate-to-severe aortic regurgitation | Diastolic inflation worsens regurgitant flow and LV volume overload. |
| Absolute / major | Aortic dissection | Balloon movement can extend the dissection or cause rupture. |
| Absolute / major | Severe PAD preventing safe access | High risk of limb ischemia, vascular injury, or failed placement. |
| Relative | Uncontrolled bleeding or severe coagulopathy | Large-bore arterial access and anticoagulation can worsen bleeding. |
| Relative | Aortic aneurysm with mural thrombus | Risk of embolization or aortic injury. |
| Relative | Severe vasodilatory shock or sepsis | IABP provides limited benefit when low SVR is the dominant problem. |
| Relative | Severe uncontrolled HTN | Higher vascular and aortic complication risk. |
Correct position
- Proximal tip 2-3 cm distal to left subclavian artery
- Distal balloon above renal arteries
- CXR marker near aortic knob/carina level
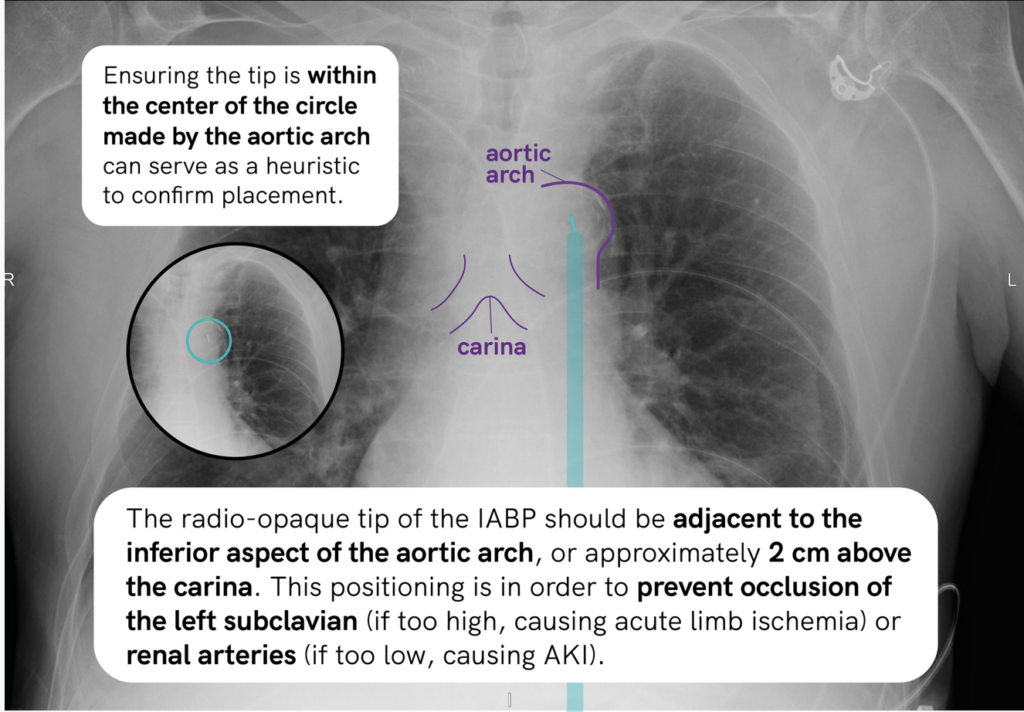
Too proximal
- Can obstruct left subclavian
- Left arm ischemia/weak left radial pulse
Too distal
- Can compromise renal, mesenteric, or visceral flow
- Rising Cr, low UOP, abdominal pain
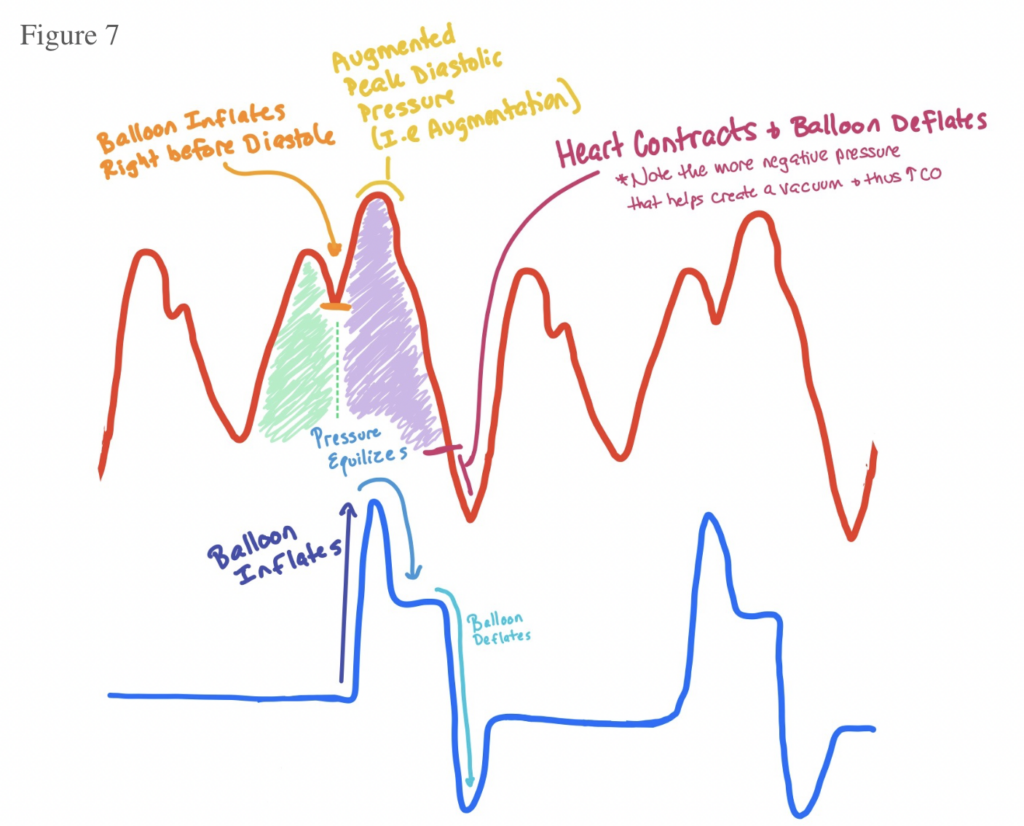
Good timing
- Inflate at dicrotic notch
- Deflate just before systole
- Augmented diastolic pressure should exceed native systolic pressure
- Assisted systolic pressure should be lower than unassisted systolic pressure
- Assisted end-diastolic pressure should be lower than unassisted EDP
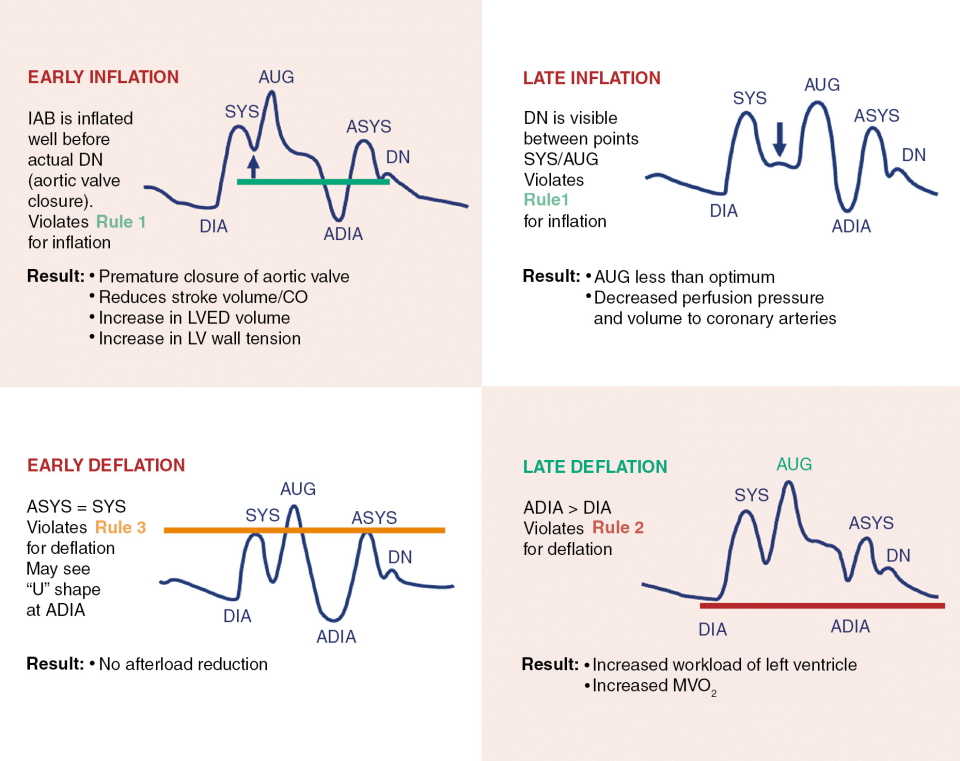
Timing problems
Late inflation
- Low diastolic augmentation
- Poor coronary perfusion
- Fix: inflate earlier
Early inflation
- Balloon inflates before systole ends
- Increases afterload
- Fix: delay inflation
Late deflation
- High assisted EDP
- Delayed/widened systolic upstroke
- Increases afterload and myocardial O2 demand
- Fix: deflate earlier
Early deflation
- Loss of diastolic augmentation
- Less afterload reduction
- Fix: delay deflation slightly
Daily management questions
- Why is the IABP still in?
- Is MAP, lactate, UOP, ischemia, and end-organ function improving?
- Is timing appropriate?
- Is there limb ischemia or bleeding?
- Is anticoagulation appropriate?
- Should we continue, wean, remove, or escalate?
Monitoring
IABP is not enough if
- Persistent hypotension
- Rising lactate
- Worsening renal/liver function
- Escalating pressors/inotropes
- Persistent pulmonary edema
- Low CI or high filling pressures despite support
- Ongoing ischemia
- Recurrent malignant arrhythmias from low output
Escalation options
- LV-predominant shock: consider Impella/stronger LV support
- Biventricular failure or severe hypoxemia: consider VA-ECMO/combined support
- RV-predominant shock: RV support strategy, treat underlying cause
- Unclear shock: PA catheter + shock team
Weaning
Criteria
- Stable MAP without escalating pressors/inotropes
- Improving lactate
- Improving UOP/end-organ function
- No active ischemia
- Definitive therapy completed or no longer needed
- Stable respiratory status
- Acceptable filling pressures/CO if PA catheter present
Typical wean
- 1:1 = full support
- 1:2 = initial wean
- 1:3 = minimal support
- Remove if perfusion remains stable
Watch during wean
- MAP
- Lactate
- UOP
- Ischemia
- Pressor/inotrope needs
- Filling pressures/CI if available
References
- Kantrowitz, A., Tjonneland, S., Freed, P. S., Phillips, S. J., Butner, A. N., & Sherman, J. L. (1968). Initial clinical experience with intraaortic balloon pumping in cardiogenic shock. JAMA, 203(2), 113–118. https://doi.org/10.1001/jama.1968.03140020075014
- Thiele, H., Zeymer, U., Neumann, F. J., Ferenc, M., Olbrich, H. G., Hausleiter, J., Richardt, G., Hennersdorf, M., Empen, K., Fuernau, G., Desch, S., Eitel, I., Hambrecht, R., Lauer, B., Böhm, M., Ebelt, H., Schneider, S., Schuler, G., Werdan, K., & IABP-SHOCK II Trial Investigators. (2012). Intraaortic balloon support for myocardial infarction with cardiogenic shock. New England Journal of Medicine, 367(14), 1287–1296. https://doi.org/10.1056/NEJMoa1208410
- Thiele, H., Zeymer, U., Thelemann, N., Neumann, F. J., Hausleiter, J., Abdel-Wahab, M., Meyer-Saraei, R., Fuernau, G., Eitel, I., Hambrecht, R., Böhm, M., Werdan, K., Felix, S. B., Hennersdorf, M., Schneider, S., Ouarrak, T., Desch, S., & IABP-SHOCK II Trial Investigators. (2019). Intraaortic balloon pump in cardiogenic shock complicating acute myocardial infarction: Long-term 6-year outcome of the randomized IABP-SHOCK II trial. Circulation, 139(3), 395–403. https://doi.org/10.1161/CIRCULATIONAHA.118.038201
- Ferguson, J. J., Cohen, M., Freedman, R. J., Stone, G. W., Miller, M. F., Joseph, D. L., & Ohman, E. M. (2001). The current practice of intra-aortic balloon counterpulsation: Results from the Benchmark Registry. Journal of the American College of Cardiology, 38(5), 1456–1462. https://doi.org/10.1016/S0735-1097(01)01553-4
- Parissis, H., Graham, V., Lampridis, S., Lau, M., Hooks, G., & Mhandu, P. C. (2016). IABP: History-evolution-pathophysiology-indications: What we need to know. Journal of Cardiothoracic Surgery, 11, 122. https://doi.org/10.1186/s13019-016-0513-0
- Naidu, S. S., Baran, D. A., Jentzer, J. C., Hollenberg, S. M., van Diepen, S., Basir, M. B., Grines, C. L., Diercks, D. B., Hall, S., Kapur, N. K., Kent, W., Sinha, S. S., Thiele, H., Zweck, E., & Henry, T. D. (2022). SCAI SHOCK stage classification expert consensus update: A review and incorporation of validation studies. Journal of the Society for Cardiovascular Angiography & Interventions, 1(1), 100008. https://doi.org/10.1016/j.jscai.2021.100008
- Gillespie, L. E., Grunau, B., & Reynolds, J. C. (2024). The intra-aortic balloon pump: A focused review of physiology, indications, complications, and transport considerations. Journal of the Society for Cardiovascular Angiography & Interventions, 3(8), 101063. https://doi.org/10.1016/j.jscai.2024.101063