Basel + Brugada + Vereckei Criteria
Basel Criteria
1. Clinical high-risk feature for VT present?
Examples prior MI, structural heart disease, prior VT, severe cardiomyopathy
2. Lead II time to first peak > 40 ms?
3. aVR time to first peak > 40 ms?
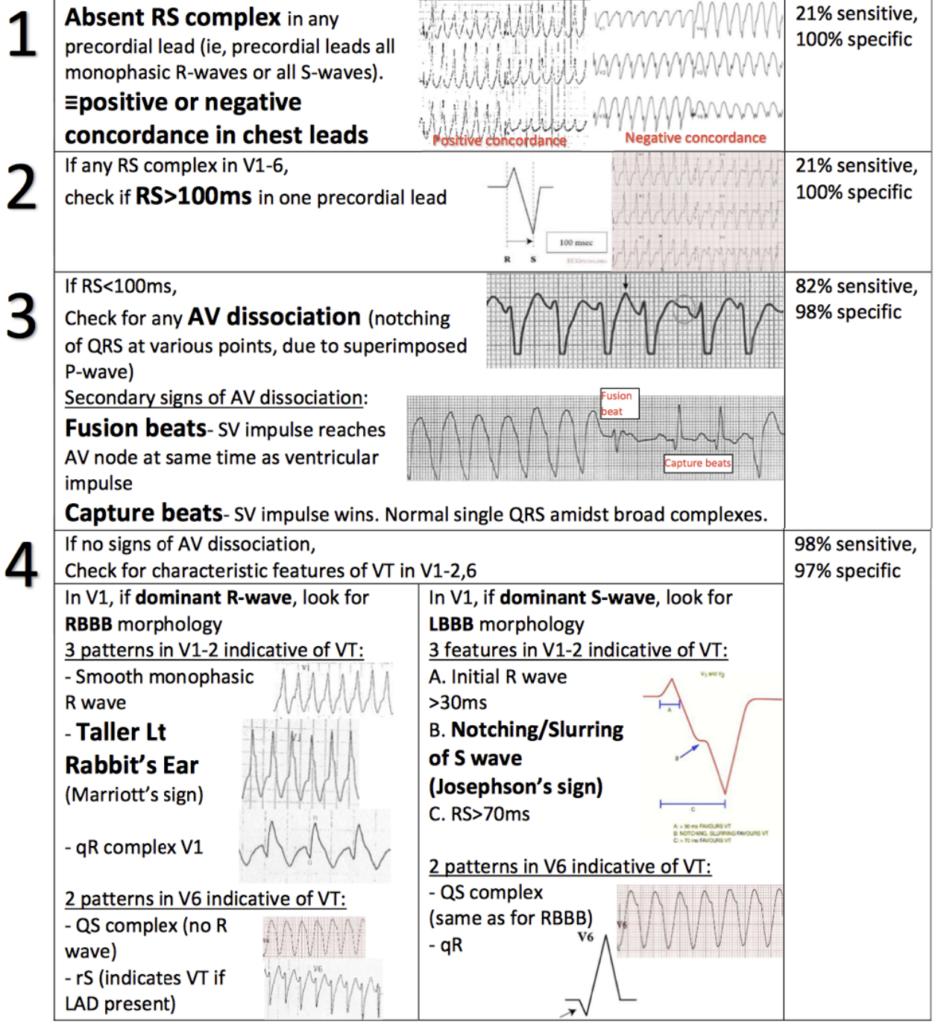
Brugada Criteria
1. No RS complex in all precordial leads?
2. RS interval > 100 ms in any precordial lead?
3. AV dissociation present?
4. Morphology criteria for VT met?
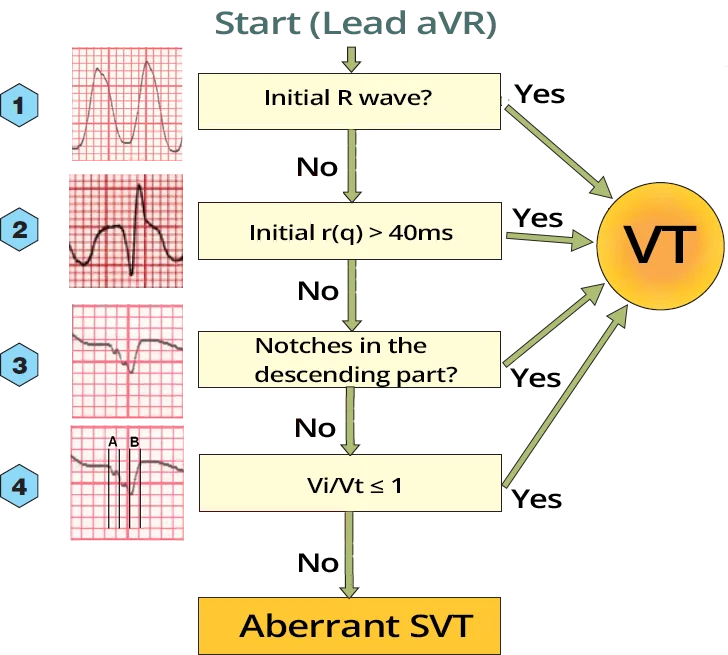
Vereckei Criteria
1. Initial R wave in aVR?
2. Initial r or q wave in aVR ≥ 40 ms?
3. Notching on the downstroke of a predominantly negative QRS in aVR?
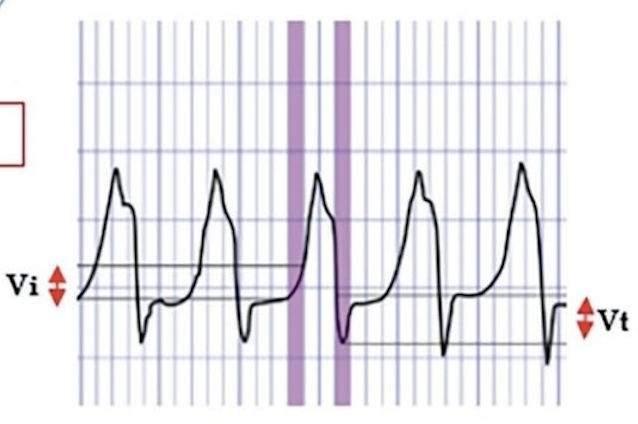
4. Vi/Vt ≤ 1?
Initial ventricular activation slower than terminal portion
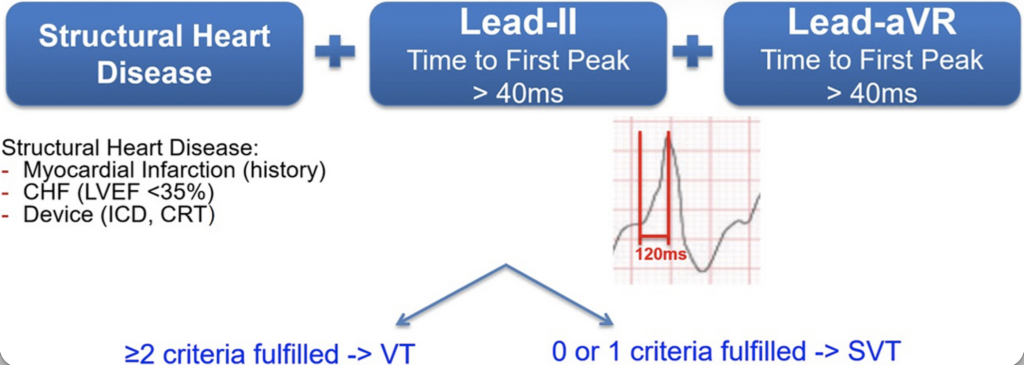
Basel Algorithm
- 2022 multicenter study proposing the Basel algorithm to differentiate VT from SVT with aberrancy in a wide-complex tachycardia
- VT diagnosed if at least 2 of 3 criteria are present
- High-risk (MI, EF<35%, ICD/CRT, other high risk structural disease)
- Lead II time to peak >40ms
- Lead aVR time to peak >40ms
- In derivation and validation cohorts the algorithm showed ~92–93% sensitivity and ~89–90% specificity for VT
- Diagnostic accuracy comparable to Brugada and Vereckei algorithms but significantly faster to apply in usability testing
Brugada Criteria
If any are + then assume VT
- Absence of RS complex in all precordial leads (V1–V6)
- If every QRS is either monophasic R or QS → VT
- RS interval >100 ms in any precordial lead
- Measure from R onset to S nadir
- AV dissociation present
- P waves independent of QRS
- Morphologic VT criteria
- Evaluate QRS morphology in V1/V2 and V6 for VT patterns
Vereckei (aVR) Algorithm
If any are + then assume VT
- Initial R wave in aVR
- Initial r or q wave in aVR ≥40 ms
- Notching on the downstroke of a predominantly negative QRS in aVR
- Vi/Vt ≤1 (initial ventricular activation slower than terminal portion)